S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- 2021-22 Headcount Enrollment by College Level Gender and Race EthnicityDocument1 pagină2021-22 Headcount Enrollment by College Level Gender and Race EthnicityUploadedbyHaroldGaterÎncă nu există evaluări
- Best of The Best Spartanburg Winners 2022Document1 paginăBest of The Best Spartanburg Winners 2022UploadedbyHaroldGaterÎncă nu există evaluări
- Justin L. Smith StatementDocument4 paginiJustin L. Smith StatementUploadedbyHaroldGaterÎncă nu există evaluări
- Tenn. State Rep. Torrey Harris ComplaintDocument1 paginăTenn. State Rep. Torrey Harris ComplaintUploadedbyHaroldGaterÎncă nu există evaluări
- Letter From Miss. AG To Jackson MayorDocument2 paginiLetter From Miss. AG To Jackson MayorUploadedbyHaroldGaterÎncă nu există evaluări
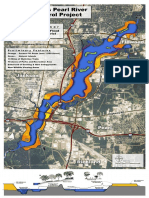
- One Lake ProjectDocument1 paginăOne Lake ProjectUploadedbyHaroldGaterÎncă nu există evaluări
- Letter To Gov. Tate Reeves On House Bill 382 FinalDocument2 paginiLetter To Gov. Tate Reeves On House Bill 382 FinalUploadedbyHaroldGaterÎncă nu există evaluări
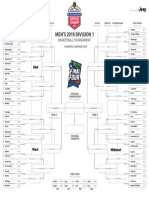
- 2019 NCAA Tournament BracketDocument1 pagină2019 NCAA Tournament BracketUSA TODAY Network100% (1)
- Proposed Mississippi Sports Betting RulesDocument21 paginiProposed Mississippi Sports Betting RulesUploadedbyHaroldGaterÎncă nu există evaluări
- National Transportation Safety Board Aviation Accident Preliminary ReportDocument4 paginiNational Transportation Safety Board Aviation Accident Preliminary ReportUploadedbyHaroldGaterÎncă nu există evaluări
- Mueller ReportDocument448 paginiMueller ReportStefan Becket95% (165)
- 2019 Mississippi Sales Tax HolidayDocument4 pagini2019 Mississippi Sales Tax HolidayUploadedbyHaroldGaterÎncă nu există evaluări
- Jay-Z, Yo Gotti Lawsuit Against Top Mississippi Prison OfficialDocument11 paginiJay-Z, Yo Gotti Lawsuit Against Top Mississippi Prison OfficialUploadedbyHaroldGater100% (2)
- 2019 NCAA Women's Basketball Tournament BracketDocument1 pagină2019 NCAA Women's Basketball Tournament BracketUSA TODAY NetworkÎncă nu există evaluări
- Speech by U.S. Judge Carlton ReevesDocument16 paginiSpeech by U.S. Judge Carlton ReevesUploadedbyHaroldGater100% (1)
- Stephanie Coleman Vs City of JacksonDocument13 paginiStephanie Coleman Vs City of JacksonUploadedbyHaroldGaterÎncă nu există evaluări
- Sample Ballot - 2018 General ElectionDocument13 paginiSample Ballot - 2018 General ElectionUploadedbyHaroldGaterÎncă nu există evaluări
- Simpson Co. Chancery Clerk IndictmentDocument1 paginăSimpson Co. Chancery Clerk IndictmentUploadedbyHaroldGaterÎncă nu există evaluări
- Hinds County District Attorney Press ReleaseDocument2 paginiHinds County District Attorney Press ReleaseUploadedbyHaroldGaterÎncă nu există evaluări
- Brandon Amphitheater Bag PolicyDocument1 paginăBrandon Amphitheater Bag PolicyUploadedbyHaroldGaterÎncă nu există evaluări
- Notice of ClaimDocument3 paginiNotice of ClaimUploadedbyHaroldGater0% (1)
- Beth Poff Zoo LetterDocument3 paginiBeth Poff Zoo LetterUploadedbyHaroldGaterÎncă nu există evaluări
- Yall Politics Survey ResultsDocument2 paginiYall Politics Survey ResultsUploadedbyHaroldGaterÎncă nu există evaluări
- Harrison Response To PEERDocument8 paginiHarrison Response To PEERBracey HarrisÎncă nu există evaluări
- David Watkins IndictmentDocument2 paginiDavid Watkins IndictmentUploadedbyHaroldGaterÎncă nu există evaluări
- 03-26-18 Remember Mississippi Exhibits #MssenDocument33 pagini03-26-18 Remember Mississippi Exhibits #MssenRuss LatinoÎncă nu există evaluări
- 03-26-18 Remember Mississippi Chris McDaniel Complaint #MssenDocument31 pagini03-26-18 Remember Mississippi Chris McDaniel Complaint #MssenRuss LatinoÎncă nu există evaluări
- McMullin Lawsuit Supplement Against MHPDocument4 paginiMcMullin Lawsuit Supplement Against MHPUploadedbyHaroldGaterÎncă nu există evaluări
- 2018 Measuring Up To The ModelDocument118 pagini2018 Measuring Up To The ModelUploadedbyHaroldGaterÎncă nu există evaluări
- Tony and Kayla Lindsey vs. Rankin County School DistrictDocument10 paginiTony and Kayla Lindsey vs. Rankin County School DistrictUploadedbyHaroldGaterÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Lab Test Results 7 2015Document3 paginiLab Test Results 7 2015Antzee Dancee0% (1)
- Host ModulationDocument17 paginiHost ModulationIbrar HumayunÎncă nu există evaluări
- ICD-11 An International Classification of DiseasesDocument11 paginiICD-11 An International Classification of DiseasesVictoria HavrylivÎncă nu există evaluări
- Pfeiffer 5 Ppts Chapter05 - The Psychology of Injury (Student Copy)Document13 paginiPfeiffer 5 Ppts Chapter05 - The Psychology of Injury (Student Copy)api-287615830Încă nu există evaluări
- Desi Elage: High Cholestrol Level in Blood (Khoon Main Cholesterol Ka Level Barh Jae)Document7 paginiDesi Elage: High Cholestrol Level in Blood (Khoon Main Cholesterol Ka Level Barh Jae)Irshad HussainÎncă nu există evaluări
- The Advanced Trauma Life Support Course: A History of Its Development and Review of Related LiteratureDocument5 paginiThe Advanced Trauma Life Support Course: A History of Its Development and Review of Related LiteratureAlphonse ThangapradeepÎncă nu există evaluări
- Comprehensive Clinical Nephrology 7th Edition AL Grawany 2024Document1.547 paginiComprehensive Clinical Nephrology 7th Edition AL Grawany 2024rozhansedikÎncă nu există evaluări
- The Poppelreuter Figure Visual PerceptualDocument4 paginiThe Poppelreuter Figure Visual PerceptualIcaroÎncă nu există evaluări
- Pulse Diagnosis of Chinese MedicineDocument69 paginiPulse Diagnosis of Chinese MedicineYanikdj100% (3)
- PDEA S Register 2-14 FormDocument12 paginiPDEA S Register 2-14 FormAngelito BALUYOT JRÎncă nu există evaluări
- Pathophysiology of Congestive Heart FailureDocument3 paginiPathophysiology of Congestive Heart Failuretinayko100% (1)
- Clikstar Dispositivo Administrador InsulinaDocument11 paginiClikstar Dispositivo Administrador InsulinaHenry SilvaÎncă nu există evaluări
- NCM 102 Care of Mother, Child, and Population Group at Risk or With ProblemsDocument33 paginiNCM 102 Care of Mother, Child, and Population Group at Risk or With ProblemsAyman DaudÎncă nu există evaluări
- Clinical Research As A CarreerDocument37 paginiClinical Research As A Carreerrahil khanÎncă nu există evaluări
- Basics of Stem Cell TransplantDocument46 paginiBasics of Stem Cell TransplantNarendra Bhattarai100% (5)
- Factors in The Relationship Between Epilepsy and Behavioral DisordersDocument19 paginiFactors in The Relationship Between Epilepsy and Behavioral DisordersEdya YopiÎncă nu există evaluări
- Shy Doc Gave Good Face: Case StudyDocument11 paginiShy Doc Gave Good Face: Case StudyIkkoÎncă nu există evaluări
- Aaos Pediatric 2020Document57 paginiAaos Pediatric 2020ABUBAKER ZANBOUZIÎncă nu există evaluări
- Lesions of The Motor PathwayDocument28 paginiLesions of The Motor PathwaykehindekolapoÎncă nu există evaluări
- Differential Diagnosis of Complex Liver Cysts.: Poster No.: Congress: Type: AuthorsDocument20 paginiDifferential Diagnosis of Complex Liver Cysts.: Poster No.: Congress: Type: Authorsrmo.rsusÎncă nu există evaluări
- Standard Operating Procedure For Literature SerchesDocument8 paginiStandard Operating Procedure For Literature SerchesboimziiÎncă nu există evaluări
- ErythromycinDocument1 paginăErythromycinKenneth Robert Abrantes0% (1)
- PBL Rickets Student GuideDocument4 paginiPBL Rickets Student GuideAhmed MostafaÎncă nu există evaluări
- Meropenem Drug StudyDocument2 paginiMeropenem Drug StudyKullin Rain100% (1)
- Department of Labor: Form300Document1 paginăDepartment of Labor: Form300USA_DepartmentOfLaborÎncă nu există evaluări
- ARI Control ProgrammeDocument13 paginiARI Control ProgrammeArun George50% (8)
- Spondilitis TBDocument14 paginiSpondilitis TBaswad 0008Încă nu există evaluări
- Parkinson - S Disease Case PresentationDocument39 paginiParkinson - S Disease Case PresentationAnonymous dpxYTE0% (1)
- Textbook of Pleural Diseases (2008)Document673 paginiTextbook of Pleural Diseases (2008)Alexandra NicaÎncă nu există evaluări