S-ar putea să vă placă și
- National Building Code of India 2016Document4 paginiNational Building Code of India 2016xahidlala100% (2)
- Key Performance Indicators - KPIs - For Learning and TeachingDocument4 paginiKey Performance Indicators - KPIs - For Learning and Teachingxahidlala0% (1)
- Planning Roles and PolesDocument17 paginiPlanning Roles and PolesxahidlalaÎncă nu există evaluări
- Revised By-Laws Amendment 210518Document29 paginiRevised By-Laws Amendment 210518xahidlalaÎncă nu există evaluări
- PSDP 2017-18 PDFDocument90 paginiPSDP 2017-18 PDFxahidlalaÎncă nu există evaluări
- University of Putra Research - Proposal - TemplateDocument4 paginiUniversity of Putra Research - Proposal - Templatexahidlala0% (1)
- Gantt Chart/ Work Plan For The Project "Upgradation of Infrastructure Facilities Nca"Document1 paginăGantt Chart/ Work Plan For The Project "Upgradation of Infrastructure Facilities Nca"xahidlalaÎncă nu există evaluări
- Annex-II Quarter ReviewDocument1 paginăAnnex-II Quarter ReviewxahidlalaÎncă nu există evaluări
- Finland PHD Proposal FormatDocument2 paginiFinland PHD Proposal Formatxahidlala50% (2)
- Luminaire Design PSDF Student ProgressDocument1 paginăLuminaire Design PSDF Student ProgressxahidlalaÎncă nu există evaluări
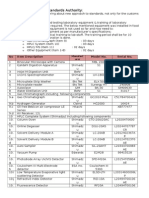
- Calibration of Food Testing Laboratory EquipmentDocument2 paginiCalibration of Food Testing Laboratory EquipmentxahidlalaÎncă nu există evaluări
- Makuleke Community Library: Sharing To Learn - M.I.TDocument1 paginăMakuleke Community Library: Sharing To Learn - M.I.TxahidlalaÎncă nu există evaluări
- Gwathmey Siegel Building and Projects 1965-2000Document167 paginiGwathmey Siegel Building and Projects 1965-2000Tedy UrsuleanuÎncă nu există evaluări
- RCC Design of A Mosque DomeDocument32 paginiRCC Design of A Mosque DomexahidlalaÎncă nu există evaluări
- Ricardo Porro Hidalgo 1925Document24 paginiRicardo Porro Hidalgo 1925xahidlalaÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Daftar Harga Pengujian Dan Kalibrasi Alat KesehatanDocument3 paginiDaftar Harga Pengujian Dan Kalibrasi Alat KesehatanVIDYA VIRA PAKSYA PUTRAÎncă nu există evaluări
- Sri Ramachandra University Application-09Document5 paginiSri Ramachandra University Application-09Mohammed RaziÎncă nu există evaluări
- Postpartum Abdominal PainDocument4 paginiPostpartum Abdominal PainPinto ModakÎncă nu există evaluări
- NGT PowerpointDocument19 paginiNGT Powerpointسانو روديلÎncă nu există evaluări
- 3 s2.0 B9780323555128001769 Main PDFDocument65 pagini3 s2.0 B9780323555128001769 Main PDFAdrian CaballesÎncă nu există evaluări
- Tumors of External EarDocument10 paginiTumors of External Earsavin1996100% (2)
- MSU-Iligan Institute of Technology: Nursing Health Assessment IDocument2 paginiMSU-Iligan Institute of Technology: Nursing Health Assessment IBianca Mikaela DosdosÎncă nu există evaluări
- M104 - ExamDocument8 paginiM104 - ExamChrystal Anne Flores CorderoÎncă nu există evaluări
- OB Med 2023 FinalDocument98 paginiOB Med 2023 FinalBelinda ELISHAÎncă nu există evaluări
- 198-Article Text-400-2-10-20210427Document8 pagini198-Article Text-400-2-10-20210427rachmatrizqaÎncă nu există evaluări
- Pharmacology For Nurses: A Pathophysiologic Approach: Fifth EditionDocument31 paginiPharmacology For Nurses: A Pathophysiologic Approach: Fifth Editionadni_wgÎncă nu există evaluări
- 0003IADDocument12 pagini0003IADRika AzyenelaÎncă nu există evaluări
- Dra Juson Labor & DeliveryDocument153 paginiDra Juson Labor & DeliveryaringkinkingÎncă nu există evaluări
- De Quervains TenosynovitisDocument2 paginiDe Quervains TenosynovitisomboÎncă nu există evaluări
- Forearm FractureDocument21 paginiForearm FractureBagus Yudha PratamaÎncă nu există evaluări
- Acute Bronchitis - FinalDocument28 paginiAcute Bronchitis - FinalJied100% (6)
- Final Paper Nanomedicine AgentsDocument16 paginiFinal Paper Nanomedicine Agentsapi-610430199Încă nu există evaluări
- Fundamentals of Using MMSDocument6 paginiFundamentals of Using MMSJoe100% (1)
- Acute CervicitisDocument9 paginiAcute CervicitisVicobeingoÎncă nu există evaluări
- 1) - Picture of Varicose Vein: Not Venogram B/C Leg Was UlceratedDocument8 pagini1) - Picture of Varicose Vein: Not Venogram B/C Leg Was Ulceratedhus100Încă nu există evaluări
- AJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Document13 paginiAJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Ana PadillaÎncă nu există evaluări
- Will The Speed of COVID-19-vaccine Development Reset Industry NormsDocument7 paginiWill The Speed of COVID-19-vaccine Development Reset Industry NormsraytjanÎncă nu există evaluări
- Auricular AcupunctureDocument16 paginiAuricular AcupunctureRamiro GuerreroÎncă nu există evaluări
- II MOCK TEST Questions OnlyDocument46 paginiII MOCK TEST Questions OnlyazitaaaaaÎncă nu există evaluări
- All-Cause Mortality and Malaria in African Children: Trends and ControversiesDocument32 paginiAll-Cause Mortality and Malaria in African Children: Trends and ControversiesBesong MichaelÎncă nu există evaluări
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterDocument4 paginiNewly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterJonas BagasÎncă nu există evaluări
- 1 s2.0 S0883540320304605 MainDocument4 pagini1 s2.0 S0883540320304605 MainSavÎncă nu există evaluări
- cl-DUTIES AND RESPONSIBILITIES OF LAB PERSONNELSDocument2 paginicl-DUTIES AND RESPONSIBILITIES OF LAB PERSONNELSRazel Ann Elagio100% (2)
- Health Assessment in Nursing Weber 5th Edition Test BankDocument9 paginiHealth Assessment in Nursing Weber 5th Edition Test BankSpencerMoorenbds100% (35)
- KONSULTA 073123 v1Document124 paginiKONSULTA 073123 v1Substationsix MalaboncpsÎncă nu există evaluări