S-ar putea să vă placă și
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- PSR ChartDocument1 paginăPSR ChartCSilva16Încă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Bare & Dundes 2004Document6 paginiBare & Dundes 2004CSilva16Încă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Injectabletechniquefordirectprovisionalrestoration PDFDocument5 paginiInjectabletechniquefordirectprovisionalrestoration PDFCSilva16Încă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Breaking Down The Barriers: The Gut Microbiome, Intestinal Permeability and Stress-Related Psychiatric DisordersDocument20 paginiBreaking Down The Barriers: The Gut Microbiome, Intestinal Permeability and Stress-Related Psychiatric DisordersCSilva16Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Immune Privilege of The Oral MucosaDocument8 paginiThe Immune Privilege of The Oral MucosaCSilva16Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Inhorn - InfectiousD Kopie - Artigo PDFDocument31 paginiInhorn - InfectiousD Kopie - Artigo PDFCSilva16Încă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- BIAS. Confounding and Effect ModificationDocument10 paginiBIAS. Confounding and Effect ModificationCSilva16Încă nu există evaluări
- Modulo1 William FarrDocument3 paginiModulo1 William FarrCSilva16Încă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- WHO - Ebola Haemorrhagic Fever.Document3 paginiWHO - Ebola Haemorrhagic Fever.CSilva16Încă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Radio Astronomy in SokendaiDocument19 paginiRadio Astronomy in SokendaiIan AnimÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- ResearchMethodology EKDocument238 paginiResearchMethodology EKAlejandra Martínez KandaÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Evaluation Method With The Use of Literacy Intervention To Detect Deception in AdvertisingDocument44 paginiEvaluation Method With The Use of Literacy Intervention To Detect Deception in AdvertisingHannson Kent NamocÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- pr2 Exam POINTERSDocument4 paginipr2 Exam POINTERSAivan LantapeÎncă nu există evaluări
- Lumax DK Automobile IndustryDocument27 paginiLumax DK Automobile IndustryJatin Pahuja100% (2)
- DLL Researchproject EditedDocument7 paginiDLL Researchproject EditedNemwel Quiño CapolÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Technological Forecasting & Social Change: Kuo-Pin Yang, Christine Chou, Yu-Jen ChiuDocument12 paginiTechnological Forecasting & Social Change: Kuo-Pin Yang, Christine Chou, Yu-Jen Chiumesay83Încă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Structure of The Research PaperDocument36 paginiStructure of The Research PaperPaul MccartneyÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Yoga As A Method of Personal Development by Danica LepojevicDocument9 paginiYoga As A Method of Personal Development by Danica LepojevicDanica Ivanovska LepojevicÎncă nu există evaluări
- B PharmacyDocument2 paginiB Pharmacysrinidhi2allÎncă nu există evaluări
- Inquiry Vs ResearchDocument19 paginiInquiry Vs ResearchAntonio Jarligo Compra71% (14)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Impact of Mobile Phone Usage On Academic Performance Among Secondary School Students in Taraba State, Nigeria 2Document9 paginiImpact of Mobile Phone Usage On Academic Performance Among Secondary School Students in Taraba State, Nigeria 2AKINYEMI ADISA KAMORU100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- Birkenholtsz & Simon - 2022 - Ignorance and Uncertainty in Environmental Decision-MakingDocument8 paginiBirkenholtsz & Simon - 2022 - Ignorance and Uncertainty in Environmental Decision-MakingSandra Rodríguez CastañedaÎncă nu există evaluări
- Elements of A Research ProposalDocument17 paginiElements of A Research ProposalDetektiv Aliff33% (3)
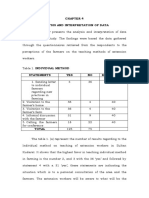
- Analysis and Interpretation of DataDocument8 paginiAnalysis and Interpretation of DataRohaina MamariongÎncă nu există evaluări
- Niños Porno TallerDocument34 paginiNiños Porno TallerRoger Inzunza100% (1)
- 2 ND Homeless Assessment ReportDocument82 pagini2 ND Homeless Assessment ReportWICKED MERCY100% (1)
- 6CN010 Dissertation Module Guide Sept 12 B2 2012-13 (BCAS SL)Document7 pagini6CN010 Dissertation Module Guide Sept 12 B2 2012-13 (BCAS SL)Malaravan GaneshamoorthyÎncă nu există evaluări
- Perten DA 7250 - Moisture in Wooden BoardsDocument4 paginiPerten DA 7250 - Moisture in Wooden BoardsaaaqÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Lateral Stability of Long Precast Concrete BeamsDocument12 paginiLateral Stability of Long Precast Concrete BeamsTaiCheong Lee100% (1)
- Reference Books For IAS General Studies Preliminary ExaminationDocument6 paginiReference Books For IAS General Studies Preliminary Examinationshettymithun91912Încă nu există evaluări
- Gebissa Dori Final Thesis After DefenceDocument69 paginiGebissa Dori Final Thesis After DefenceMuktar AbdulkerimÎncă nu există evaluări
- Beh 020 Motivation Assessment ScaleDocument2 paginiBeh 020 Motivation Assessment ScaleMarta YantiÎncă nu există evaluări
- Problems Faced by University Campus Students Due To Load SheddingDocument6 paginiProblems Faced by University Campus Students Due To Load SheddingEMMANUEL OSEI100% (1)
- Challenges Faced by Human Resources in Software IndustryDocument35 paginiChallenges Faced by Human Resources in Software IndustryAyush SinghalÎncă nu există evaluări
- Chemistry Quiz Chapter 1 Form 4Document2 paginiChemistry Quiz Chapter 1 Form 4Mohd Norihwan100% (5)
- School of Engineering and Architecture Baguio City: TopicsDocument13 paginiSchool of Engineering and Architecture Baguio City: TopicsEmd Quidasol100% (1)
- Diagnostic vs. Prognostic Assessment: Getting To The Good StuffDocument19 paginiDiagnostic vs. Prognostic Assessment: Getting To The Good StuffSanjay ChandwaniÎncă nu există evaluări
- What Is Comparative Study?: By: Syed Aftab Hassan BukhariDocument8 paginiWhat Is Comparative Study?: By: Syed Aftab Hassan BukhariJade Ligan EliabÎncă nu există evaluări
- NLM - ControllingDocument8 paginiNLM - ControllingNa NaÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)