Documente Academic
Documente Profesional
Documente Cultură
Diare
Încărcat de
Sena Rian RizardiTitlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
Diare
Încărcat de
Sena Rian RizardiDrepturi de autor:
Formate disponibile
Kl i egman: Nelson Textbook of Pediatri cs, 18th ed.
Copyright 2007 Saunders, An Imprint of Elsevier
Chapter 337 Acute Gastroenteri ti s in Chi l dren
Zulfiqar Ahmed Bhutta
The term gastroenteritis denotes infections of the gastrointestinal tract caused by bacterial, viral, or parasitic pathogens (Tables
337-1 to 337-3 [1] [2] [3]). Many of these infections are food-borne illnesses. The most common manifestations are diarrhea
and vomiting, which may also be associated with systemic features such as abdominal pain and fever. The term
gastroenteritis captures the bulk of infectious cases of diarrhea. The term diarrheal disorders is more commonly used to
denote infectious diarrhea in public health settings, although several noninfectious causes of gastrointestinal illness with
vomiting and/or diarrhea are well recognized ( Table 337-4 ).
TABLE 337-1--Food-borne Illnesses (Bacterial)
ETIOLOGY
INCUBATION
PERIOD
SIGNS AND
SYMPTOMS
DURATION
OF
ILLNESS
ASSOCIATED
FOODS
LABORATORY
TESTING TREATMENT
Bacillus anthracis 2 days to
weeks
Nausea, vomiting,
malaise, bloody
diarrhea, acute
abdominal pain
Weeks Insufficiently
cooked
contaminated
meat
Blood
Penicillin is
first choice for
naturally
acquired
gastrointestinal
anthrax.
Ciprofloxacin
is second
option.
Bacillus cereus
(preformed
enterotoxin)
16 hr Sudden onset of
severe nausea and
vomiting. Diarrhea
may be present.
24 hr Improperly
refrigerated
cooked or
fried rice,
meats
Normally a
clinical diagnosis.
Clinical
laboratories do
not routinely
identify this
organism. If
indicated, send
stool and food
specimens to
reference
laboratory for
culture and toxin
identification.
Supportive care
Bacillus cereus
(diarrheal toxin)
1016 hours Abdominal cramps,
watery diarrhea,
nausea.
2448 hr Meats, stews,
gravies,
vanilla sauce
Testing not
necessary, self-
limiting (consider
testing food and
stool for toxin in
outbreaks).
Supportive care
Brucella abortus, B.
melitensis, and B.
suis
721 days Fever, chills,
sweating, weakness,
headache, muscle
and joint pain,
diarrhea, bloody
stools during acute
phase
Weeks Raw milk,
goat cheese
made from
unpasteurized
milk,
contaminated
meats
Blood culture and
positive serology
Acute: Rifampin and
doxycycline daily for
6wk. Infections
with complications
require combination
therapy with
rifampin,
tetracycline, and an
aminoglycoside.
Campylobacter
jejuni
25 days Diarrhea, cramps,
fever, and vomiting;
diarrhea may be
bloody.
210 days Raw and
undercooked
poultry,
unpasturized
milk,
contaminated
water
Routine stool
culture;
Campylobacter
requires special
media and
incubation at 42
C to grow.
Supportive care.
For severe cases,
antibiotics such as
erythromycin and
quinolones may be
indicated early in
the diarrheal
disease. Guillain-
Barr syndrome can
be a sequela.
Clostridium
botulinum
1272 hr Vomiting, diarrhea,
blurred vision,
Variable
(from days
Home-canned
foods with a
Stool, serum, and
food can be
Supportive care.
Botulism antitoxin is
Page 1 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
children and adults
(preformed toxin)
diplopia, dysphagia,
and descending
muscle weakness
to months).
Can be
complicated
by
respiratory
failure and
death.
low acid
content,
improperly
canned
commercial
foods, home-
canned or
fermented
fish, herb-
infused oils,
baked
potatoes in
aluminium foil,
cheese sauce,
bottled garlic,
foods held
warm for
extended
periods of
time (e.g., in a
warm oven)
tested for toxin.
Stool and food
can also be
cultured for the
organism. These
tests can be
performed at
some state
health
department
laboratories and
CDC.
helpful if given early
in the course of the
illness. Contact the
state health
department. The
24-hour number for
state health
departments to call
is (700) 4887100.
Clostridium
botulinuminfants
330 days In infants <12 mo,
lethargy, weakness,
poor feeding,
constipation,
hypotonia, poor head
control, poor gag and
sucking reflex
Variable Honey, home-
canned
vegetables
and fruits,
corn syrup
Stool, serum, and
food can be
tested for toxin.
Stool and food
can also be
cultured for the
organism. These
tests can be
performed at
some state
health
department
laboratories and
CDC.
Supportive care.
Botulism immune
globulin can be
obtained from the
Infant Botulism
Prevention
Program, Health
and Human
Services, California
(510-540-2646),
Botulinum antitoxin
is generally not
recommended for
infants.
Clostridium
perfringens toxin
816 hr Watery diarrhea,
nausea, abdominal
cramps; fever is rare.
2448 hr Meats,
poultry, gravy,
dried or
precooked
foods, time-
and/or
temperature-
abused food
Stools can be
tested for
enterotoxin and
cultured for
organism.
Because
Clostridium
perfringens can
normally be
found in stool,
quantitative
cultures must be
done.
Supportive care.
Antibiotics not
indicated.
Enterohemorrhagic
E. coli (EHEC)
including E. coli
O157 : H7 and
other Shiga toxin
producing E. coli
(STEC)
18 days Severe diarrhea that
is often bloody,
abdominal pain and
vomiting. Usually,
little or no fever is
present. More
common in children
<4 yr old.
510 days Undercooked
beef
especially
hamburger,
unpasteurized
milk and juice,
raw fruits and
vegetables
(e.g., sprouts),
salami
(rarely), and
contaminated
water
Stool culture; E.
coli O157 : H7
requires special
media to grow. If
E. coli O157 : H7
is suspected,
specific testing
must be
requested. Shiga
toxin testing may
be done using
commercial kits;
positive isolates
should be
forwarded to
public health
laboratories for
confirmation and
serotyping.
Supportive care,
monitor renal
function,
hemoglobin, and
platelets closely. E.
coli O157 : H7
infection is also
associated with
hemolytic uremic
syndrome (HUS),
which can cause
lifelong
complications.
Studies indicate that
antibiotics may
promote the
development of
HUS.
Enterotoxigenic E.
coli (ETEC)
13 days Watery diarrhea,
abdominal cramps,
some vomiting
3 to >7 days Water or food
contaminated
with human
feces
Stool culture.
ETEC requires
special laboratory
techniques for
Supportive care.
Antibiotics are
rarely needed
except in severe
Page 2 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
identification. If
suspected, must
request specific
testing.
cases.
Recommended
antibiotics include
TMP-SMX and
quinolones.
Listeria
monocytogenes
948 hr for
gastrointestinal
symptoms, 2
6 wk for
invasive
disease
Fever, muscle aches,
and nausea or
diarrhea. Pregnant
women may have
mild flu-like illness,
and infection can lead
to premature delivery
or stillbirth. Elderly or
immunocompromised
patients may have
bacteremia or
meningitis.
Variable Fresh soft
cheeses,
unpasteurized
milk,
inadequately
pasteurized
milk, ready-to-
eat deli
meats, hot
dogs
Blood or
cerebrospinal
fluid cultures.
Asymptomatic
fecal carriage
occurs; therefore,
stool culture
usually not
helpful. Antibody
to listerolysin O
may be helpful to
identify outbreak
retrospectively.
Supportive care and
antibiotics;
Intravenous
ampicillin, penicillin,
or TMP-SMX are
recommended for
invasive disease.
At birth and
infancy
Infants infected from
mother at risk for
sepsis or meningitis.
Salmonella spp. 13 days Diarrhea, fever,
abdominal cramps,
vomiting. S. typhi and
S. paratyphi produce
typhoid with insidious
onset characterized
by fever, headache,
constipation, malaise,
chills, and myalgia;
diarrhea is
uncommon, and
vomiting is not usually
severe.
47 days Contaminated
eggs, poultry,
unpasteurized
milk or juice,
cheese,
contaminated
raw fruits and
vegetables
(alfalfa
sprouts,
melons). S.
typhi
epidemics are
often related
to fecal
contamination
of water
supplies or
street-vended
foods.
Routine stool
cultures
Supportive care.
Other than for S.
typhi and S.
paratyphi, antibiotics
are not indicated
unless there is
extra-intestinal
spread, or the risk of
extra-intestinal
spread, of the
infection. Consider
ampicillin,
gentamicin, TMP-
SMX, or quinolones
if indicated. A
vaccine exists for S.
typhi.
Shigella spp. 2448 hr Abdominal cramps,
fever, and diarrhea.
Stools may contain
blood and mucus.
47 days Food or water
contaminated
with human
fecal material.
Usually
person-to-
person
spread, fecal-
oral
transmission.
Ready-to-eat
foods touched
by infected
food workers,
e.g., raw
vegetables,
salads,
sandwiches.
Routine stool
cultures
Supportive care.
TMP-SMX
recommended in
the U. S. if
organism is
susceptible;
nalidixic acid or
other quinolones
may be indicated if
organism is
resistant, especially
in developing
countries.
Staphylococcus
aureus (preformed
enterotoxin)
16 hr Sudden onset of
severe nausea and
vomiting. Abdominal
cramps. Diarrhea and
fever may be present.
2448 hrs Unrefrigerated
or improperly
refrigerated
meats, potato
and egg
salads, cream
pastries.
Normally a
clinical diagnosis.
Stool, vomitus,
and food can be
tested for toxin
and cultured if
indicated.
Supportive care.
Vibrio cholerae
(toxin)
2472 hr Profuse watery
diarrhea and
vomiting, which can
lead to severe
37 days.
Causes life-
threatening
dehydration.
Contaminated
water, fish,
shellfish,
street-vended
Stool culture;
Vibrio cholerae
requires special
media to grow. If
Supportive care
with aggressive oral
and intravenous
rehydration. In
Page 3 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
dehydration and
death within hours
food typically
from Latin
America or
Asia
V. cholerae is
suspected, must
request specific
testing.
cases of confirmed
cholera, tetracycline
or doxycycline is
recommended for
adults, and TMP-
SMX for children
(<8 yr).
Vibrio
parahaemolyticus
248 hr Watery diarrhea,
abdominal cramps,
nausea, vomiting.
25 days Undercooked
or raw
seafood, such
as fish,
shellfish
Stool cultures.
Vibrio
parahaemolyticus
requires special
media to grow. If
V.
parahaemolyticus
is suspected,
must request
specific testing.
Supportive care.
Antibiotics are
recommended in
severe cases:
tetracycline,
doxycycline,
gentamicin, and
cefotaxime.
Vibrio vulnificus 17 days Vomiting, diarrhea,
abdominal pain,
bactermia, and wound
infections. More
common in the
immunocompromised,
or in patients with
chronic liver disease
(presenting with
bullous skin lesions).
Can be fatal in
patients with liver
disease and the
immunocompromised.
28 days Undercooked
or raw
shellfish,
especially
oysters, other
contaminated
seafood, and
open wounds
exposed to
seawater
Stool, wound, or
blood cultures.
Vibrio vulnificus
requires special
media to grow. If
V. vulnificus is
suspected, must
request specific
testing.
Supportive care and
antibiotics;
tetracycline,
doxycycline, and
ceftazidime are
recommended.
Yersinia
enterocolytica and
Y.
pseudotuberculosis
2448 hr Appendicitis-like
symptoms (diarrhea
and vomiting, fever,
and abdominal pain)
occur primarily in
older children and
young adults. May
have a scarlitiniform
rash or erythema
nodosum with Y.
pseudotuberculosis.
13 wk,
usually self-
limiting
Undercooked
pork,
unpasteurized
milk, tofu,
contaminated
water.
Infection has
occurred in
infants whose
caregivers
handled
chitterlings.
Stool, vomitus, or
blood culture.
Yersinia requires
special media to
grow. If
suspected, must
request specific
testing. Serology
is available in
research and
reference
laboratories.
Supportive care. If
septicemia or other
invasive disease
occurs, antibiotic
therapy with
gentamicin or
cefotaxime
(doxycycline and
ciprofloxacin also
effective).
From: Department of Health and Human Services, Centers for Disease Control and Prevention: Diagnosis and management of
foodbourne illnesses. MMWR 2004:53:79.
TABLE 337-2--Food-borne Illnesses (Viral)
CDC, Centers for Disease Control and Prevention;TMP-SMX, trimethoprim-sulfamethoxazole.
ETIOLOGY
INCUBATION
PERIOD SIGNS AND SYMPTOMS
DURATION
OF
ILLNESS
ASSOCIATED
FOODS
LABORATORY
TESTING TREATMENT
Hepatitis A 28 days
average (15
50 days)
Diarrhea, dark urine,
jaundice, and flu-like
symptoms, i.e., fever,
headache, nausea, and
abdominal pain
Variable, 2
wk3 mo
Shellfish harvested
from contaminated
waters, raw
produce,
contaminated
nated drinking
water, uncooked
foods and cooked
foods that are not
reheated after
contact with
infected food
handler
Increase in ALT,
billirubin. Positive
IgM and anti
hepatitis A
antibodies.
Supportive
care.
Prevention with
immunization.
Noroviruses
(and other
1248 hr Nausea, vomiting,
abdominal cramping,
1260 hr Shellfish, fecally
contaminated
Routine RT-PCR
and EM on fresh
Supportive
care such as
Page 4 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
caliciviruses) diarrhea, fever, myalgia,
and some headache.
Diarrhea is more prevalent
in adults and vomiting is
more prevalent in children.
Prolonged asymptomatic
excretion possible.
foods, ready-to-eat
foods touched by
infected food
workers (salads,
sandwiches, ice,
cookies, fruit)
unpreserved stool
samples. Clinical
diagnosis,
negative bacterial
cultures. Stool is
negative for
WBCs.
rehydration.
Good hygiene.
Rotavirus 13 days Vomiting, watery diarrhea,
low-grade fever.
Temporary lactose
intolerance may occur.
Infants and children,
elderly, and
immunocompromised are
especially vulnerable.
48 days Fecally
contaminated
foods. Ready-to-
eat foods touched
by infected food
workers (salads,
fruits).
Identification of
virus in stool via
immunoassay
Supportive
care. Severe
diarrhea may
require fluid
and electrolyte
replacement.
Other viral
agents
(astroviruses,
adenoviruses,
parvoviruses)
1070 hr Nausea, vomiting,
diarrhea, malaise,
abdominal pain,
headache, fever
29 days Fecally
contaminated
foods. Ready-to-
eat foods touched
by infected food
workers. Some
shellfish.
Identification of the
virus in early acute
stool samples.
Serology.
Commercial ELISA
kits are now
available for
adenoviruses and
astroviruses.
Supportive
care, usually
mild, self-
limiting. Good
hygiene.
From: Department of Health and Human Services, Centers for Disease Control and Prevention: Diagnosis and management of
foodbourne illnesses. MMWR 2004:53:9.
TABLE 337-3--Food-borne Illnesses (Parasitic)
ALT, alanine aminotransferase; ELISA, enzyme linked immunoserbent assay; EM, electron microscopy; IgM, immunoglobulin
M;RT-PCR, reverse transcriptose polymerase chain reaction; WBCs, white blood cells.
ETIOLOGY
INCUBATION
PERIOD
SIGNS AND
SYMPTOMS
DURATION
OF
ILLNESS
ASSOCIATED
FOODS
LABORATORY
TESTING TREATMENT
Angiostrongylus
cantonensis
1 wk to1mo Severe headaches,
nausea, vomiting,
neck stiffness,
paresthesias,
hyperesthesias,
seizures, and other
neurologic
abnormalities
Several
weeks to
several
months
Raw or
undercooked
intermediate
hosts (e.g.,
snails or
slugs),
infected
paratenic
(transport)
hosts (e.g.,
crabs,
freshwater
shrimp), fresh
produce
contaminated
with
intermediate or
transport hosts
Examination of
CSF for elevated
pressure, protein,
leukocytes, and
eosinophils;
serologic testing
using ELISA to
detect antibodies
to Angiostrongylus
cantonensis
Supportive care.
Repeat lumbar
punctures and use of
corticosteroid therapy
may be used for more
severely ill patients.
Cryptosporidium 210 days Diarrhea (usually
watery), stomach
cramps, upset
stomach, slight fever
May be
remitting
and
relapsing
over weeks
to months
Any uncooked
food or food
contaminated
by an ill food
handler after
cooking;
drinking water
Request specific
examination of the
stool for
Cryptosporidium.
May need to
examine water or
food.
Supportive care, self-
limited. If severe
consider paromomycin
for 7 days. For children
aged 111 yr, consider
nitazoxanide for 3
days.
Cyclospora
cayetanensis
114 days,
usually at
least 1 wk
Diarrhea (usually
watery), loss of
appetite, substantial
loss of weight,
stomach cramps,
nausea, vomiting,
fatigue
May be
remitting
and
relapsing
over weeks
to months
Various types
of fresh
produce
(imported
berries,
lettuce)
Request specific
examination of the
stool for
Cyclospora. May
need to examine
water or food.
TMP-SMX for 7 days.
Entamoeba 23 days to Diarrhea (often May be Any uncooked Examination of Metronidazole and a
Page 5 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
histolytica 14 wk bloody), frequent
bowel movements,
lower abdominal pain
protracted
(several
weeks to
several
months)
food or food
contaminated
by an ill food
handler after
cooking;
drinking water
stool for cysts and
parasitesmay
need at least 3
samples. Serology
for long-term
infections.
luminal agent
(iodoquinol or
paromomycin)
Giardia lamblia 12 wk Diarrhea, stomach
cramps, gas, weight
loss
Days to
weeks
Any uncooked
food or food
contaminated
by an ill food
handler after
cooking;
drinking water.
Examination of
stool for ova and
parasitesmay
need at least 3
samples.
Metronidazole
Toxoplasma
gondii
523 days Generally
asymptomatic, 20%
may develop cervical
lymphadenopathy
and/or a flu-like
illness. In
immunocompromised
patients: central
nervous system
(CNS) disease,
myocarditis, or
pneumonitis is often
seen.
Months Accidental
ingestion of
contaminated
substances
(e.g., soil
contaminated
with cat feces
on fruits and
vegetables),
raw or partly
cooked meat
(especially
pork, lamb, or
venison)
Isolation of
parasites from
blood or other
body fluids;
observation of
parasites in patient
specimens via
microscopy or
histology.
Detection of
organisms is rare;
serology
(reference
laboratory needed)
can be a useful
adjunct in
diagnosing
toxoplasmosis.
However, IgM
antibodies may
persist for 618
mo and thus may
not necessarily
indicate recent
infection. PCR of
bodily fluids. For
congenital
infection: isolation
of T. gondii from
placenta, umbilical
cord, or infant
blood. PCR of
white blood cells,
CSF, or amniotic
fluid, or IgM and
IgA serology,
performed by a
reference
laboratory.
Asymptomatic healthy,
but infected, persons
do not require
treatment. Spiramycin
or pyrimethamine plus
sulfadiazine may be
used for pregnant
women.
Pyrimethamine plus
sulfadiazine may be
used for
immunocompromised
persons, in specific
cases. Pyrimethamine
plus sulfadiazine (with
or without steroids)
may be given for
ocular disease when
indicated. Folinic acid
is given with
pyrimethamine plus
sulfadiazine to
counteract bone
marrow suppression.
Toxoplasma
gondii
(congenital
infection)
In infants at
birth
Treatment of the
mother may reduce
severity and/or
incidence of
congenital infection.
Most infected infants
have few symptoms at
birth. Later, they will
generally develop
signs of congenital
toxoplasmosis (mental
retardation, severely
impaired eyesight,
cerebral palsy,
seizures), unless the
infection is treated
Months Passed from
mother (who
acquired acute
infection
during
pregnancy) to
child
Trichinella
spiralis
12 days for
initial
symptoms;
Acute:nausea,
diarrhea, vomiting,
fatigue, fever,
Months Raw or
undercooked
contaminated
Positive serology
or demonstration
of larvae via
Supportive care plus
mebendazole or
albendazole
Page 6 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
others begin
28 wk after
infection
abdominal discomfort
followed by muscle
soreness, weakness,
and occasional
cardiac and
neurologic
complications
meat, usually
pork or wild
game meat
(e.g., bear or
moose)
muscle biopsy.
Increase in
eosinophils.
From: Department of Health and Human Services, Centers for Disease Control and Prevention: Diagnosis and management of
foodbourne illnesses. MMWR 2004:53:910.
TABLE 337-4--Food-borne Illnesses (Noninfectious)
CSF, cerebrospinal fluid; ELISA, enzyme linked immunoserbent assay; IgM, immunoglobulin M;PCR, polymerase chain
reaction; TMP-SMX, trimethoprim-sulfamethoxazole.
ETIOLOGY
INCUBATION
PERIOD SIGNS AND SYMPTOMS
DURATION
OF
ILLNESS
ASSOCIATED
FOODS
LABORATORY
TESTING TREATMENT
Antimony 5 min8 hr
usually <1 hr
Vomiting, metallic taste Usually
self-limited
Metallic
container
Identification of
metal in
beverage or
food
Supportive
care
Arsenic Few hours Vomiting, colic, diarrhea Several
days
Contaminated
food
Urine. May
cause
eosinophilia
Gastric lavage,
BAL
(dimercaprol)
Cadmium 5 min8 hr
usually <1 hr
Nausea, vomiting, myalgia,
increase in salivation,
stomach pain
Usually
self-limited
Seafood,
oysters, clams,
lobster, grains,
peanuts
Identification of
metal in food
Supportive
care
Ciguatera fish
poisoning
(ciguatera toxin)
26 hr Gl:abdominal pain, nausea,
vomiting, diarrhea
Days to
weeks to
months
A variety of
large reef fish:
grouper, red
snapper,
amberjack,
and barracuda
(most
common)
Radioassay for
toxin in fish or a
consistent
history
Supportive
care, IV
mannitol.
Children more
vulnerable.
3 hr Neurologic:paresthesias,
reversal of hot or cold, pain,
weakness
25 days Cardiovascular:bradycardia,
hypotension, increase in T
wave abnormalities
Copper 5 min8 hr
usually <1 hr
Nausea, vomiting, blue or
green vomitus
Usually
self-limited
Metallic
container
Identification of
metal in
beverage or
food
Supportive
care
Mercury 1 wk or longer Numbness, weakness of
legs, spastic paralysis,
impaired vision, blindness,
coma. Pregnant women and
the developing fetus are
especially vulnerable.
May be
protracted
Fish exposed
to organic
mercury,
grains treated
with mercury
fungicides
Analysis of
blood, hair
Supportive
care
Mushroom toxins,
short-acting
(museinol,
muscarine,
psilocybin, Coprius
artemetaris,
ibotenic acid)
<2 hr Vomiting, diarrhea,
confusion, visual
disturbance, salivation,
diaphoresis, hallucinations,
disulfiram-like reaction,
confusion, visual
disturbance.
Self-limited Wild
mushrooms
(cooking may
not destroy
these toxins)
Typical
syndrome and
mushroom
identified or
demonstration of
the toxin
Supportive
care
Mushroom toxins,
long-acting
(amanitin)
48 hr
diarrhea; 24
48 hr liver
failure
Diarrhea, abdominal cramps,
leading to hepatic and renal
failure
Often fatal Mushrooms Typical
syndrome and
mushroom
identified and/or
demonstration of
the toxin
Supportive
care, life-
threatening,
may need life
support
Page 7 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
Nitrite poisoning 12 hr Nausea, vomiting, cyanosis,
headache, dizziness,
weakness, loss of
consciousness, chocolate-
brown colored blood
Usually
self-limited
Cured meats,
any
contaminated
foods, spinach
exposed to
excessive
nitrification
Analysis of the
food, blood
Supportive
care,
methylene blue
Pesticides
(organophosphates
or carbamates
Few min to
few hours
Nausea, vomiting,
abdominal cramps, diarrhea,
headache, nervousness,
blurred vision, twitching,
convulsions, salivation and
meiosis
Usually
self-limited
Any
contaminated
food
Analysis of the
food, blood
Atropine;2-
PAM
(Pralidoxime)
is used when
atropine is not
able to control
symptoms and
is rarely
necessary in
carbamate
poisoning.
Puffer fish
(tetrodotoxin)
<30 min Parasthesias, vomiting,
diarrhea, abdominal pain,
ascending paralysis,
respiratory failure
Death
usually in
46 hr
Puffer fish Detection of
tetrodotoxin in
fish
Life-
threatening,
may need
respiratory
support
Scombroid
(histamine)
1 min3 hr Flushing, rash, burning
sensation of skin, mouth and
throat, dizziness, urticaria,
parasthesias
36 hr Fish:bluefin,
tuna, skipjack,
mackerel,
marlin, escolar,
and mahi mahi
Demonstration
of histamine in
food or clinical
diagnosis
Supportive
care,
antihistamines
Shellfish toxins
(diarrheic,
neurotoxic,
amnesic)
Diarrheic
shellfish
poisoning
(DSP) 30
min to 2 hr
Nausea, vomiting, diarrhea,
and abdominal pain
accompanied by chills,
headache, and fever
Hours to 2
3 days
A variety of
shellfish,
primarily
mussels,
oysters,
scallops, and
shellfish from
the Florida
coast and the
Gulf of Mexico
Detection of the
toxin in shellfish;
high-pressure
liquid
chromatography
Supportive
care, generally
self-limiting.
Elderly are
especially
sensitive to
ASP
Neurotoxic
shellfish
poisoning
(NSP) few
min to hours
Tingling and numbness of
lips, tongue, and throat,
muscular aches, dizziness,
reversal of the sensations of
hot and cold, diarrhea, and
vomiting
Amnesic
shellfish
poisoning
(ASP)24
48 hr
Vomiting, diarrhea,
abdominal pain and
neurologic problems such as
confusion, memory loss,
disorientation, seizure, coma
Shellfish toxins
(paralytic shellfish
poisoning)
30 min3 hr Diarrhea, nausea, vomiting
leading to parasthesias of
mouth, lips, weakness,
dysphasia, dysphonia,
respiratory paralysis
Days Scallops,
mussels,
clams, cockles
Detection of
toxin in food or
water where fish
are located;
high-pressure
liquid
chromatography
Life-
threatening,
may need
respiratory
support
Sodium fluoride Few min to 2
hr
Salty or soapy taste,
numbness of mouth,
vomiting, diarrhea, dilated
pupils, spasms, pallor,
shock, collapse
Usually
self-limited
Dry foods
(e.g., dry milk,
flour, baking
powder, cake
mixes)
contaminated
with sodium
fluoride
containing
insecticides
and
rodenticides
Testing of
vomitus or
gastric
washings.
Analysis of the
food.
Supportive
care
Page 8 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
Thallium Few hours Nausea, vomiting, diarrhea,
painful parathesias, motor
polyneuropathy, hair loss
Several
days
Contaminated
food
Urine, hair Supportive
care
Tin 5 min8 hr
usually <1 hr
Nausea, vomiting, diarrhea Usually
self-limited
Metallic
container
Analysis of the
food
Supportive
care
Vomitoxin Few min to 3
hr
Nausea, headache,
abdominal pain, vomiting
Usually
self-limited
Grains such as
wheat, corn,
barley
Analysis of the
food
Supportive
care
Zinc Few hours Stomach cramps, nausea,
vomiting, diarrhea, myalgias
Usually
self-limited
Metallic
container
Analysis of the
food, blood and
feces, saliva or
urine
Supportive
care
From: Department of Health and Human Services, Centers for Disease Control and Prevention: Diagnosis and management of
foodbourne illnesses. MMWR 2004:53:1112.
EPIDEMIOLOGY OF CHILDHOOD DIARRHEA
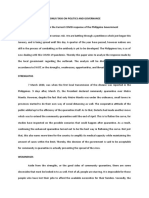
Diarrheal disorders in childhood account for a large proportion (18%) of childhood deaths, with an estimated 1.8 million deaths
per year globally. The World Health Organization (WHO) suspects that there are >700 million episodes of diarrhea annually in
children <5 yr of age in developing countries. While global mortality may be declining, the overall incidence of diarrhea remains
unchanged at about 3.2 episodes per child year ( Fig. 337-1 ). In the UnitedStates,thereare1.5millionoutpatientvisitsfor
gastroenteritis, 200,000 hospitalizations, and 300 deaths annually.
Globally, it was estimated in 1999 that Shigella infections may lead to 600,000 deaths per year of children <5 yr of age, or a
quarter to a third of all diarrhea-related mortality in this age group. Rates of hospitalization and deaths due to Shigella
infections, especially S. dysenteriae type 1, the most severe form of shigellosis, may be declining; recent estimates are
160,000 deaths. Rotavirus infections (the most common identifiable viral cause of gastroenteritis in all children) account for at
least 35% of severe and potentially fatal watery diarrhea episodes, with an estimated 500,000 deaths per year worldwide due
to rotavirus infections.
The decline in diarrheal mortality, despite the lack of significant changes in incidence, is the result of improved case
management of diarrhea, as well as improved nutrition of infants and children. These interventions have included widespread
home- and hospital-based oral rehydration therapy, as well as improved nutritional management of children with diarrhea.
Persistently high rates of diarrhea among young children, despite intensive efforts at control, are of particular concern. There is
very little information on the long-term consequences of diarrheal diseases, especially persistent or prolonged diarrhea and
malnutrition. Diarrheal illnesses may have a significant impact on psychomotor and cognitive development in young children.
Early and repeated episodes of childhood diarrhea during periods of critical development, especially when associated with
malnutrition, co-infections, and anemia may have long-term effects on linear growth, as well as on physical and cognitive
functions.
ETIOLOGY OF DIARRHEA
Gastroenteritis is due to infection acquired through the feco-oral route or by ingestion of contaminated food or water.
Gastroenteritis is associated with poverty, poor environmental hygiene, and development indices. Enteropathogens that are
Figure 337-1 Global trends in diarrhea incidence.
Page 9 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook of ...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
infectious in a small inoculum (Shigella, Escherichia coli, noroviruses, rotavirus, Giardia lamblia, Cryptosporidium parvum,
Entamoeba histolytica) can be transmitted by person-to-person contact, whereas others such as cholera are generally a
consequence of contamination of food or water supply (see Tables 337-1 to 337-3 [1] [2] [3]). In the United States, rotavirus
and the noroviruses (small round viruses such as Norwalk-like virus and caliciviruses) are the most common viral agents,
followed by enteric adenoviruses and astroviruses (see Table 337-2 ). Food-borne outbreaks of diarrhea in the United States
are most commonly due to Salmonella and Campylobacter species, followed much less often by Shigella, Cryptosporidium, E.
coli 0157: H7, Yersinia, Listeria, Vibrio, and Cyclospora species, in that order. Salmonella, Shigella, and, most notably, the
various diarrhea-producing E. coli organisms are the most common pathogens in developing countries (see Table 337-1 ).
Clostridium difficile (by toxin production) is linked to antibiotic-associated diarrhea and pseudomembranous colitis, although
most cases of antibiotic-associated diarrhea in children are not due to C. difficile. C. difficile negative antibiotic associated
hemorrhagic colitis in adults may be due to cytotoxin-producing Klebsiella oxytoca.
In developed countries, episodes of infectious diarrhea can occur through seasonal exposure to organisms such as rotavirus or
exposure to pathogens in settings of close contact (e.g., daycare centers). Children in developing countries become infected
with a diverse group of bacterial and parasitic pathogens, whereas all children in developed as well as developing countries
acquire rotavirus and, in many cases, other viral enteropathogens as well as G. lamblia and C. parvum in their 1st 5 yr of life.
PATHOGENESIS OF INFECTIOUS DIARRHEA
Pathogenesis and severity of bacterial disease depend on whether organisms have preformed toxins (Staphylococcus aureus,
Bacillus cereus), produce toxins, or are invasive and on whether they replicate in food. Enteropathogens can lead to either an
inflammatory or noninflammatory response in the intestinal mucosa.
Enteropathogens elicit noninflammatory diarrhea through enterotoxin production by some bacteria, destruction of villus
(surface) cells by viruses, adherence by parasites, and adherence and/or translocation by bacteria. Inflammatory diarrhea is
usually caused by bacteria that directly invade the intestine or produce cytotoxins with consequent fluid, protein, and cells
(erythrocytes, leukocytes) that enter the intestinal lumen. Some enteropathogens possess more than one virulence property.
Some viruses, such as rotavirus, target the microvillous tips of the enterocytes and can enter the cells by either direct invasion
or calcium-dependent endocytosis. This can result in villus shortening and loss of enterocyte absorptive surface through cell
shortening and loss of microvilli ( Fig. 337-2 ).
Most bacterial pathogens elaborate enterotoxins; the rotavirus protein NSP4 acts as a viral enterotoxin. Bacterial enterotoxins
can selectively activate enterocyte intracellular signal transduction, and can also affect cytoskeletal rearrangements with
subsequent alterations in the water and electrolyte fluxes across enterocytes. Upregulation of these pathways results in
Figure 337-2 Pathogenesis of rotavirus infection and diarrhea. ER, endoplasmic reticulum; TJ , tight junction. (Adapted from Ramig RF: Pathogenesis of intestinal
and systemic rotavirus infection. J Virol 2004;78:1021310220.)
Page 10 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
inhibition of NaCl-coupled transport and increased efflux of chloride, resulting, in turn, in net secretion and loss of water into the
intestinal lumen ( Fig. 337-3 ). Coupled transport of sodium to glucose and amino acids is largely unaffected. The nitric oxide
pathway can also be involved, as endogenous nitric oxide production is significantly higher in infectious compared with
noninfectious diarrhea.
Enterotoxigenic E. Coli (ETEC) colonizes and adheres to enterocytes of the small bowel via its surface fimbriae (pili) and
induces hypersecretion of fluids and electrolytes into the small intestine through one of two toxins: the heat-labile enterotoxin
(LT) or the heat-stable enterotoxin. LT is structurally similar to the Vibrio cholera toxin, and activates adenylate cyclase,
resulting in an increase in intracellular cyclic guanosine monophosphate (cGMP) (see Fig. 337-3 ). In contrast, Shigella spp.
cause gastroenteritis via a superficial invasion of colonic mucosa, which they invade through M cells located over Peyer
patches. After phagocytosis, a series of events occurs, including apoptosis of macrophages, multiplication and spread of
bacteria into adjacent cells, release of inflammatory mediators (interleukin [IL]-1 and IL-8), transmigration of neutrophils into the
lumen of the colon, neutrophil necrosis and degranulation, further breach of the epithelial barrier, and mucosal destruction
( Fig. 337-4 ).
Figure 337-3 Mechanism of cholera toxin. (Adapted from Thapar M, Sanderson IR: Diarrhoea in children: An interface between developing and developed countries.
Lancet 2004;363:641653; and Montes M, DuPont HL: Enteritis, enterocolitis and infectious diarrhea syndromes. In Cohen J, Powderly WG, Opal SM, et al [editors]:
Infections Diseases, 2nd ed. London, Mosby, 2004, pp 3152.)
Page 11 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
RISK FACTORS FOR GASTROENTERITIS
Major risks include environmental contamination and increased exposure to enteropathogens. Additional risks include young
age, immune deficiency, measles, malnutrition, and lack of exclusive or predominant breast-feeding. Malnutrition increases
severalfold the risk of diarrhea and associated mortality. The fraction of such infectious diarrhea deaths that are attributable to
nutritional deficiencies varies with the prevalence of deficiencies; the highest attributable fractions are in sub-Saharan Africa,
south Asia, and Andean Latin America. The risks are particularly higher with micronutrient malnutrition; in children with vitamin
A deficiency, the risk of dying from diarrhea, measles, and malaria is increased by 2024%. Zinc deficiency increases the
risk of mortality from diarrhea, pneumonia, and malaria by 1321%.
The majority of cases of diarrhea resolve within the 1st wk of the illness. A smaller proportion of diarrheal illnesses fail to
resolve and persist for >2 wk. Persistent diarrhea is defined as episodes that began acutely but last for at least 14 days. Such
episodes account for between 3% and 20% of all diarrheal episodes in children <5 yr of age and up to 50% of all diarrhea-
related deaths. Many children (especially infants and toddlers) in developing countries have frequent episodes of acute
diarrhea. Although few individual episodes persist beyond 14 days, frequent episodes of acute diarrhea can result in nutritional
compromise and may predispose these children to develop persistent diarrhea, protein-calorie malnutrition, and secondary
infections.
CLINICAL MANIFESTATION OF DIARRHEA
Most of the clinical manifestations and clinical syndromes of diarrhea are related to the infecting pathogen and the
dose/inoculum (see Tables 337-1 to 337-3 [1] [2] [3]). Additional manifestations depend on the development of complications
(such as dehydration and electrolyte imbalance) and the nature of the infecting pathogen (see Chapter 55.1 ). Usually the
ingestion of preformed toxins (such as those of Staphylococcus aureus) is associated with the rapid onset of nausea and
vomiting within 6 hr, with possible fever, abdominal cramps, and diarrhea within 872 hr. Watery diarrhea and abdominal
cramps after an 816 hr incubation period are associated with enterotoxin-producing Clostridium perfringens and Bacillus
cereus. Abdominal cramps and watery diarrhea after a 1648 hr incubation period can be associated with noroviruses, several
enterotoxin-producing bacteria, Cryptosporidium, and Cyclospora. Several organisms, including Salmonella, Shigella,
Campylobacter jejuni, Yersinia enterocolitica, enteroinvasive E. coli, and Vibrio parahaemolyticus, produce diarrhea that can
contain blood as well as fecal leukocytes in association with abdominal cramps, tenesmus, and fever; these features suggest
bacterial dysentery and fever. Bloody diarrhea and abdominal cramps after a 72120 hr incubation period are associated with
infections due to Shigella and also Shiga toxinproducing E. coli, such as E. coli 0157 : H7. Organisms associated with
dysentery or hemorrhagic diarrhea can also cause watery diarrhea alone without fever or that precedes a more complicated
course that results in dysentery.
Although many of the manifestations of acute gastroenteritis in children are nonspecific, some clinical features can help identify
major categories of diarrhea and allow rapid triage for antibiotic or specific dietary therapy (see Tables 337-1 to 337-3 [1] [2]
[3]). There is considerable overlap in the symptomatology. The positive predictive values for the features of dysentery are very
poor; however, the negative predictability for bacterial pathogens is much better in the absence of signs of dysentery. If
warranted and if facilities and resources permit, the etiology can be verified by appropriate laboratory testing.
COMPLICATIONS
Most of the complications associated with gastroenteritis are related to delays in diagnosis and delays in the institution of
appropriate therapy. Without early and appropriate rehydration, many children with acute diarrhea would develop dehydration
with associated complications (see Chapters 53 , 54 , 55 , and 68 ). These can be life-threatening in infants and young
Figure 337-4 Pathogenesis of Shigella infection and diarrhea. (Adapted from Opal SM, Keusch GT: Host responses to infection. In Cohen J, Powderly WG, Opal SM,
et al [editors]: Infections Diseases, 2nd ed. London, Mosby, 2004, pp 3152.)
Page 12 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
children. Inappropriate therapy can lead to prolongation of the diarrheal episodes, with consequent malnutrition and
complications such as secondary infections and micronutrient deficiencies (iron, zinc). In developing countries, associated
bacteremias are well-recognized complications in malnourished children with diarrhea.
Specific pathogens are associated with extra-intestinal manifestations and complications. These are not pathognomonic of the
infection nor do they always occur in close temporal association with the diarrheal episode ( Table 337-5 ).
TABLE 337-5--Extraintestinal Manifestations of Enteric Infections
MANIFESTATION
ASSOCIATED ENTERIC
PATHOGEN(S) ONSET AND PROGNOSIS
Focal infections due to systemic spread of
bacterial pathogens, including vulvovaginitis,
urinary tract infection, endocarditis,
osteomyelitis, meningitis, pneumonia, hepatitis,
peritonitis, chorioamnionitis, soft tissue infection,
and septic thrombophlebitis
All major pathogens can
cause such direct
extraintestinal infections,
including Salmonella,
Onset usually during the acute infection, but may
present subsequently. Prognosis depends on
infection site.
Shigella, Yersinia,
Campylobacter,
Clostridium difficile
Reactive arthritis Salmonella, Shigella,
Yersinia, Campylobacter,
Cryptosporidium,
Clostridium difficile
Typically occurs about 13 wk after infection.
Relapses after reinfection may develop in 1550%
of people but most children recover fully within 26
mo after the 1st symptoms appear.
Guillain-Barr syndrome Campylobacter Usually occurs a few weeks after the original
infection. Prognosis good although 1520% may
have sequelae.
Glomerulonephritis Shigella, Campylobacter,
Yersinia
Can be of sudden onset in acute, referring to a
sudden attack of inflammation, or chronic, which
comes on gradually. In most cases, the kidneys
heal with time.
IgA nephropathy Campylobacter Characterized by recurrent episodes of blood in
the urine, this condition results from deposits of the
protein immunoglobulin A (IgA) in the glomeruli.
IgA nephropathy can progress for years with no
noticeable symptoms. Men seem more likely to
develop this disorder than are women.
Erythema nodosum Yersinia, Campylobacter,
Salmonella
Although painful, is usually benign and more
commonly seen in adolescents. Resolves with 46
weeks.
Hemolytic uremia syndrome Shigella dysenteriae 1,
Escherichia coli 0157: H7,
others
Sudden onset, short-term renal failure. In severe
cases, renal failure requires several sessions of
dialysis to take over the kidney function, but most
children recover without permanent damage to
their health.
Hemolytic anemia Campylobacter, Yersinia Relatively rare complication and may have a
chronic course.
From: Department of Health and Human Services, Centers for Disease Control and Prevention: Managing acute gastroenteritis
among children. MMWR Recomm Rep 2004;53:133.
DIAGNOSIS
The diagnosis of gastroenteritis is based on clinical recognition, an evaluation of its severity by rapid assessment, and
confirmation by appropriate laboratory investigations, if indicated.
CLINICAL EVALUATION OF DIARRHEA.
The most common manifestation of gastrointestinal tract infection in children is diarrhea, abdominal cramps, and vomiting.
Systemic manifestations are varied and associated with a variety of causes. The evaluation of a child with acute diarrhea
includes:
Assess the degree of dehydration and acidosis and provide rapid resuscitation and rehydration with oral or
intravenous fluids as required ( Table 337-6 and Table 337-7 ).
Obtain appropriate contact or exposure history. This includes information on exposure to contacts with
similar symptoms, intake of contaminated foods or water, child-care center attendance, recent travel to a
diarrhea-endemic area, and use of antimicrobial agents.
Page 13 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
This clinical approach to the diagnosis and management of diarrhea in young children is a critical component of the integrated
management of childhood illness (IMCI) package that is being implemented in developing countries with high burden of
diarrhea mortality ( Fig. 337-5 ).
TABLE 337-6--Symptoms Associated with Dehydration
Clinically determine the etiology of diarrhea for institution of prompt antibiotic therapy, if indicated.
Although nausea and vomiting are nonspecific symptoms, they are indicative of infection in the upper
intestine. Fever is suggestive of an inflammatory process but also occurs as a result of dehydration or co-
infection (e.g., urinary tract infection, otitis media). Fever is common in patients with inflammatory diarrhea.
Severe abdominal pain and tenesmus are indicative of involvement of the large intestine and rectum.
Features such as nausea and vomiting and absent or low-grade fever with mild to moderate periumbilical
pain and watery diarrhea are indicative of small intestine involvement and also reduce the likelihood of a
serious bacterial infection.
SYMPTOM
MINIMAL OR NO DEHYDRATION
(<3% LOSS OF BODY WEIGHT)
MILD TO MODERATE
DEHYDRATION (39% LOSS OF
BODY WEIGHT)
SEVERE DEHYDRATION (>9%
LOSS OF BODY WEIGHT)
Mental status Well;alert Normal, fatigued or restless, irritable Apathetic, lethargic, unconscious
Thirst Drinks normally; might refuse liquids Thirsty;eager to drink Drinks poorly; unable to drink
Heart rate Normal Normal to increased Tachycardia, with bradycardia in
most severe cases
Quality of
pulses
Normal Normal to decreased Weak, thready, or impalpable
Breathing Normal Normal;fast Deep
Eyes Normal Slightly sunken Deeply sunken
Tears Present Decreased Absent
Mouth and
tongue
Moist Dry Parched
Skinfold Instant recoil Recoil in <2 sec Recoil in >2 sec
Capillary refill Normal Prolonged Prolonged;minimal
Extremities Warm Cool Cold;mottled;cyanotic
Urine output Normal to decreased Decreased Minimal
From: Department of Health and Human Services, Centers for Disease Control and Prevention: Diagnosis and management of
foodbourne illnesses. MMWR 2004:52;5.
TABLE 337-7--Summary of Treatment Based on Degree of Dehydration
Sources: Adapted from Duggan C, Santosham M, Glass RI: The management of acute diarrhea in children: Oral rehydration,
maintenance, and nutritional therapy.MMWR 1992;41 (No. RR-16):120;and World Health Organization: The treatment of
diarrhoea: a manual for physicians and other senior health workers. Geneva, Switzerland: World Health Organization, 1995.
Available at http://www.who.int/child-adolescent-health/New_Publications/CHILD_HEALTH/WHO.CDR.95.3.htm .
DEGREE OF
DEHYDRATION REHYDRATION THERAPY REPLACEMENT OF LOSSES NUTRITION
Minimal or no
dehydration
Not applicable <10 kg body weight: 60120 mL oral
rehydration solution (ORS) for each
diarrheal stool or vomiting episode;
>10 kg body weight: 120240 mL
ORS for each diarrheal stool or
vomiting episode
Continue breast-feeding,
or resume age-appropriate
normal diet after initial
hydration, including
adequate caloric intake for
maintenance[*]
Mild to moderate
dehydration
ORS, 50100 mL/kg body weight over 34
hr
Same Same
Severe
dehydration
Lactated Ringer solution or normal saline in
20 mL/kg body weight intravenous amounts
until perfusion and mental status improve;
then administer 100 mL/kg body weight
ORS over 4 hr or 5% dextrose normal
saline intravenously at twice maintenance
fluid rates
Same;if unable to drink, administer
through nasogastric tube or
administer 5% dextrose normal
saline with 20 mEq/L potassium
chloride intravenously
Same
From: Department of Health and Human Services, Centers for Disease Control and Prevention: Diagnosis and management of
foodbourne illnesses. MMWR 2004;52:133.
Page 14 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
STOOL EXAMINATION.
Microscopic examination of the stool and cultures can yield important information on the etiology of diarrhea. Stool specimens
should be examined for mucus, blood, and leukocytes. Fecal leukocytes are indicative of bacterial invasion of colonic mucosa,
although some patients with shigellosis have minimal leukocytes at an early stage of infection, as do patients infected with
Shiga toxinproducing E. coli and E. histolytica. In endemic areas, stool microscopy must include examination for parasites
causing diarrhea, such as G. lamblia and E. histolytica.
Stool cultures should be obtained as early in the course of disease as possible from children with bloody diarrhea in whom
stool microscopy indicates fecal leukocytes; in outbreaks with suspected hemolytic-uremic syndrome (HUS); and in
immunosuppressed children with diarrhea. Stool specimens for culture need to be transported and plated quickly; if the latter
is not quickly available, specimens may need to be transported in special media. The yield and diagnosis of bacterial diarrhea
can be significantly improved by using molecular diagnostic procedures such as PCR. In most previously healthy children with
uncomplicated watery diarrhea, no laboratory evaluation is needed except for epidemiologic purposes.
TREATMENT
The broad principles of management of acute gastroenteritis in children include oral rehydration therapy, enteral feeding and
diet selection, zinc supplementation, and additional therapies such as probiotics.
ORAL REHYDRATION THERAPY.
Children, especially infants, are more susceptible than adults to dehydration because of the greater basal fluid and electrolyte
requirements per kg and because they are dependent on others to meet these demands. Dehydration must be evaluated
rapidly and corrected in 46 hr according to the degree of dehydration and estimated daily requirements. A small minority of
children, especially those in shock or unable to tolerate oral fluids, require initial intravenous rehydration, but oral rehydration is
the preferred mode of rehydration and replacement of ongoing losses ( Table 337-7 and Table 337-8 ). Risks associated with
severe dehydration that may necessitate intravenous resuscitation include: age <6 mo, prematurity, chronic illness, fever >38
C if <3 mo or >39C if 336 mo, bloody diarrhea, persistent emesis, poor urine output, sunken eyes, and a depressed level of
consciousness. Although, in general, the standard WHO oral rehydration solution (ORS) is adequate, lower osmolality oral
rehydration fluids can be more effective in reducing stool output. Compared with standard ORS, lower sodium and glucose
ORS (containing 75 mEq of sodium and 75 mmol of glucose per liter, with total osmolarity of 245 mOsm per liter) reduces stool
output, vomiting, and the need for intravenous fluids without substantially increasing the risk of hyponatremia.
TABLE 337-8--Composition of Commercial Oral Rehydration Solutions (ORS) and Commonly Consumed Beverages
* Overly restricted diets should be avoided during acute diarrheal episodes. Breast-fed infants should continue to nurse ad libitumeven during acute rehydration. Infants too
weak to eat can be given milk or formula through a nasogastric tube. Lactose-containing formulas are usually well tolerated. If lactose malabsorption appears clinically
substantial, lactose-free formulas can be used. Complex carbohydrates, fresh fruits, lean meats, yogurt, and vegetables are all recommended. Carbonated drinks or
commercial juices with a high concentration of simple carbohydrates should be avoided.
Figure 337-5 Integrated management of the sick child (IMCI) protocol for the recognition and management of diarrhea in developing countries.
SOLUTION
CARBOHYDRATE
(G/L)
SODIUM
(MMOL/L)
POTASSIUM
(MMOL/L)
CHLORIDE
(MMOL/L)
BASE[*]
(MMOL/L)
OSMOLARITY
(MOSM/L)
ORS
World Health
Organization (WHO)
[2005]
13.5 75 20 65 10 245
WHO [2002] 13.5 75 20 65 30 245
WHO (1975) 20 90 20 80 30 311
European Society of
Page 15 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
Paediatric
Gastroenterology,
Hepatology and Nutrition
16 60 20 60 30 240
Enfalyte[] 30 50 25 45 34 200
Pedialyte[] 25 45 20 35 30 250
Rehydralyte[] 25 75 20 65 30 305
CeraLyte[**] 40 5090 20 NA[] 30 220
COMMONLY USED BEVERAGES (NOT APPROPRIATE FOR DIARRHEA TREATMENT)
Apple juice[] 120 0.4 44 45 N/A 730
Coca-Cola[] Classic 112 1.6 N/A N/A 13.4 650
From: Department of Health and Human Services, Centers for Disease Control and Prevention: Diagnosis and management of
foodbourne illnesses. MMWR 2004;52:133.
Cereal-based oral rehydration fluids can also be advantageous in malnourished children and can be prepared at home. Home
remedies including decarbonated soda beverages, fruit juices, and tea are not suitable for rehydration or maintenance therapy
as they have inappropriately high osmolalities and low sodium concentrations. A clinical evaluation plan and management
strategy for children with moderate to severe diarrhea is outlined in Figure 337-5 and Table 337-7 . Oral rehydration should be
given to infants and children slowly, especially if they have emesis. It can be given initially by a dropper, teaspoon, or syringe,
beginning with as little as 5 mL at a time. The volume is increased as tolerated. Replacement for emesis or stool losses is
noted in Table 337-7 . Oral rehydration can also be given by a nasogastric tube if needed; this is not the usual route.
Limitations to oral rehydration therapy include shock, an ileus, intussusception, carbohydrate intolerance (rare), severe emesis,
and high stool output (>10 mL/kg/hr).
ENTERAL FEEDING AND DIET SELECTION.
Continued enteral feeding in diarrhea aids in recovery from the episode and a continued age-appropriate diet after rehydration
is the norm. Although intestinal brush border surface and luminal enzymes can be affected in children with prolonged diarrhea,
there is evidence that satisfactory carbohydrate, protein, and fat absorption can take place on a variety of diets. Once
rehydration is complete, food should be reintroduced while oral rehydration can be continued to replace ongoing losses from
emesis or stools and for maintenance. Breast-feeding or nondiluted regular formula should be resumed as soon as possible.
Foods with complex carbohydrates (rice, wheat, potatoes, bread, and cereals), lean meats, yogurt, fruits, and vegetables are
also tolerated. Fatty foods or foods high in simple sugars (juices, carbonated sodas) should be avoided. The usual energy
density of any diet used for the therapy of diarrhea should be around 1 kcal/g, aiming to provide an energy intake of a minimum
of 100 kcal/kg/day and a protein intake of between 2 and 3 g/kg/day. In selected circumstances when adequate intake of
energy-dense food is problematic, the addition of amylase to the diet through germination techniques can also be helpful.
With the exception of acute lactose intolerance in a small subgroup, most children with diarrhea are able to tolerate milk and
lactose-containing diets. Withdrawal of milk and replacement with specialized (and expensive) lactose-free formulations are
unnecessary. Although children with persistent diarrhea are not lactose intolerant, administration of a lactose load exceeding 5
g/kg/day may be associated with higher purging rates and treatment failure. Alternative strategies for reducing the lactose load
while feeding malnourished children with prolonged diarrhea include addition of milk to cereals as well as replacement of milk
with fermented milk products such as yogurt.
Rarely, when dietary intolerance precludes the administration of cow's milkbased formulations or milk it may be necessary to
administer specialized milk-free diets such as a comminuted or blenderized chicken-based diet or an elemental formulation.
Although effective in some settings, the latter are unaffordable in most developing countries. In addition to rice-lentil
formulations, the addition of green banana or pectin to the diet has also been shown to be effective in the treatment of
persistent diarrhea. Figure 337-6 indicates a suggestive algorithm for the management of children with prolonged diarrhea in
developing countries.
* Actual or potential bicarbonate (e.g., lactate, citrate, or acetate).
Mead-J ohnson Laboratories, Princeton, New J ersey. Additional information is available at http://www.meadjohnson.com/products/cons-infant/enfalyte.html .
Ross Laboratories (Abbott Laboratories), Columbus, Ohio. Data regarding Flavored and Freezer Pop Pedialyte are identical. Additional information is available at
http://www.pedialyte.com .
Ross Laboratories (Abbott Laboratories), Columbus, Ohio. Additional information is available at
http://rpdcon40.ross.com/pn/PediatricProducts.NSF/web_Ross.com_XML_PediatricNutrition/96A5745B1183947385256A80007546E5?OpenDocument .
**
Cera Products, L. L. C., J essup, Maryland. Additional information is available at http://www.ceralyte.com/index.htm .
Not applicable.
Meeting U. S. Department of Agriculture minimum requirements.
Coca-Cola Corporation, Atlanta, Georgia. Figures do not include electrolytes that might be present in local water used for bottling. Base =phosphate.
Page 16 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
ZINC SUPPLEMENTATION.
There is strong evidence that zinc supplementation in children with diarrhea in developing countries leads to reduced duration
and severity of diarrhea and could potentially prevent 300,000 deaths. WHO and UNICEF recommend that all children with
acute diarrhea in at-risk areas should receive oral zinc in some form for 1014 days during and after diarrhea (10 mg/day for
infants <6 mo of age and 20 mg/day for those >6 mo). In addition to improving diarrhea, administration of zinc in community
settings leads to increased use of ORS and reduction in the use of antimicrobials.
ADDITIONAL THERAPIES.
The use of probiotic nonpathogenic bacteria for prevention and therapy of diarrhea has been successful in developing
countries. There are a variety of organisms (Lactobacillus, Bifidobacterium) that have a good safety record; therapy has not
been standardized and the most effective (and safe) organism has not been identified.
Antimotility agents (loperamide) are contraindicated in children with dysentery and probably have no role in the management
of acute watery diarrhea in otherwise healthy children. Similarly, antiemetic agents such as the phenothiazines are of little
value and are associated with potentially serious side effects (lethargy, dystonia, malignant hyperpyrexia). Nonetheless,
ondansetron is an effective and less toxic antiemetic agent. Because persistent vomiting may limit oral rehydration therapy, a
single sublingual dose of an oral dissolvable tablet of ondansetron (2 mg children 815 kg; 4 mg children <1530 kg; 8 mg
children >30 kg) may be given. However, most children do not require specific antiemetic therapy; careful oral rehydration
therapy is usually sufficient (see Chapter 55.1 ).
Racecadotril, an enkephalinse inhibitor, has been shown to reduce stool output in patients with diarrhea. Experience with this
drug in children is limited, and for the average child with acute diarrhea it may be unnecessary.
ANTIBIOTIC THERAPY.
Timely antibiotic therapy in select cases of diarrhea may reduce the duration and severity of diarrhea and prevent
complications ( Table 337-9 ). While these agents are important to use in specific cases, their widespread and indiscriminate
use leads to the development of antimicrobial resistance. Nitazoxanide, an anti-infective agent, has been effective in the
treatment of a wide variety of pathogens including Cryptosporidum parvum, Giardia lamblia, Entamoeba histolytica,
Blastocystis hominis, C. difficile, and rotavirus.
TABLE 337-9--Antibiotic Therapy for Infectious Diarrhea
Figure 337-6 Persistent diarrhea. NG, nasogastric tube; ORS, oral rehydration solution.
DOSE AND
Page 17 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
ORGANISM DRUG OF CHOICE
DURATION OF
TREATMENT
Shigella (severe dysentery
and EIEC dysentery)
Ciprofloxacin, ampicillin, ceftriaxone, or trimethoprim-sulfamethoxazole
(TMP-SMX).
Ceftriaxone IV, IM 50
100 mg/kg/d qd, bid 7
d
Most strains are resistant to many antibiotics. Ciprofloxacin PO 2030
mg/kg/d bid 710 d
10 mg/kg/d of TMP and
50 mg/kg/d of SMX bid
5 d
Ampicillin PO, IV 50
100 mg/kg/d qid 7 d
EPEC, ETEC, EIEC TMP-SMX or ciprofloxacin 10 mg/kg/d of TMP and
50 mg/kg/d of SMX bid
5 d
Ciprofloxacin PO 2030
mg/kg/d qid for 510 d
Salmonella No antibiotics for uncomplicated gastroenteritis in normal hosts caused
by non-typhoidal species.
See treatment of
Shigella
Treatment indicated in infants <3 mo, and patients with malignancy,
chronic GI disease, severe colitis hemoglobinopathies, or HIV infection,
and other immunoincompetent patients.
Most strains have become resistant to multiple antibiotics.
Aeromonas/Plesiomonas TMP-SMX 10 mg/kg/d of TMP and
50 mg/kg/d of SMX bid
for 5 d
Ciprofloxacin Ciprofloxacin PO 2030
mg/kg/d divided bid
710 d
Yersinia spp. Antibiotics are not usually required for diarrhea.
Deferoxamine therapy should be withheld for severe infections or
associated bacteremia. Treat sepsis as for immunocompromised hosts,
using combination therapy with parenteral doxycycline, aminoglycoside,
TMP-SMX, or fluoroquinolone.
Campylobacter jejuni Erythromycin or azithromycin Erythromycin PO, 50
mg/kg/d divided tid 5
d
Azithromycin PO, 510
mg/kg/d qid 5 d
Clostridium difficile Metronidazole (first line) PO 30 mg/kg/d divided
tid 5 d
Discontinue initiating antibiotic
Vancomycin (2nd line) PO 40 mg/kg/d qid 7
d
Entamoeba histolytica Metronidazole followed by iodoquinol or paromomycin PO 3040 mg/kg/d tid
710 d
PO 3040 mg/kg/d tid
20 d
PO 2535 mg/kg/d tid
7 d
Giardia lamblia Furazolidone or metronidazole or albendazole or quinacrine Furazolidone PO 25
mg/kg/d qid for 57 d
Metronidazole PO 30
40 mg/kg/d tid 7 d
Albendazole PO 200
mg bid 10 d
Cryptosporidium spp. Nitazoxanide PO treatment may not be needed in normal hosts. In
immunocompromised, PO immunoglobulin +aggressively treat HIV, etc.
Children 13 yr: 100
mg bid 3 d
Children 411 yr: 200
mg bid
Adults: 500 mg bid
Page 18 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
PREVENTION
In many developed countries, diarrhea due to pathogens such as Clostridum botulinum, E. coli 0157 : H7, Salmonella, Shigella,
V. cholerae, Cryptosporidium, and Cyclospora is a notifiable disease and, thus, contact tracing and source identification is
important in preventing outbreaks.
Many developing countries struggle with huge disease burdens of diarrhea where a wider approach to diarrhea prevention may
be required. Preventive strategies may be of relevance to both developed and developing countries.
PROMOTION OF EXCLUSIVE BREAST-FEEDING.
Exclusive breast-feeding (administration of no other fluids or foods for the 1st 6 mo of life) is not common. Exclusive breast-
feeding protects very young infants from diarrheal disease through the promotion of passive immunity (see Chapters 42 and
94 ) and through reduction in the intake of potentially contaminated food and water. Breast milk contains all the nutrients
needed in early infancy, and when continued during diarrhea, also diminishes the adverse impact on nutritional status.
IMPROVED COMPLEMENTARY FEEDING PRACTICES.
There is a strong inverse association between appropriate, safe complementary feeding and mortality in children age 611 mo;
malnutrition is an independent risk for the frequency and severity of diarrheal illness. Complementary foods should be
introduced at 6 mo of age while breast-feeding should continue for up to 1 yr (longer period for developing countries).
Complementary foods in developing countries are generally poor in quality and frequently heavily contaminated, thus
predisposing to diarrhea. Contamination of complementary foods can be potentially reduced through caregivers' education and
improving home food storage. Vitamin A supplementation reduces childhood mortality by 34%; improved vitamin A status
reduces the frequency of severe diarrhea.
ROTAVIRUS IMMUNIZATION.
Most infants acquire rotavirus diarrhea early in life; an effective rotavirus vaccine would have a major effect on reducing
diarrhea mortality in developing countries. In 1998, a quadrivalent Rhesus rotavirusderived vaccine was licensed in the United
States but subsequently withdrawn due to an increased risk of intussusception. Newer vaccines are approved for both
developed and developing countries and significantly reduce diarrhea mortality (see Chapters 170 , 262 ).
Other vaccines that could potentially reduce the burden of severe diarrhea and mortality in young children are vaccines against
Shigella and ETEC.
IMPROVED WATER AND SANITARY FACILITIES AND PROMOTION OF PERSONAL AND DOMESTIC HYGIENE.
Much of the reduction in diarrhea prevalence in the developed world is the result of improvement in standards of hygiene,
sanitation, and water supply. In addition, routine handwashing with plain soap in the home can reduce the incidence of diarrhea
in all environments. Behavioral change strategies through promotion of handwashing indicate that handwashing promotion and
access to soap reduces the burden of diarrhea in developing countries.
IMPROVED CASE MANAGEMENT OF DIARRHEA.
Improved management of diarrhea through prompt identification and appropriate therapy significantly reduces diarrhea
duration, its nutritional penalty, and risk of death in childhood. Improved management of acute diarrhea is a key factor in
reducing the burden of prolonged episodes and persistent diarrhea. The WHO/UNICEF recommendations to use low
osmolality ORS and zinc supplementation for the management of diarrhea, coupled with selective and appropriate use of
antibiotics, have the potential to reduce the number of diarrheal deaths among children.
Isospora spp. TMP-SMX PO 5 mg/kg/d and 25
mg/kg/d, respectively,
bid 710 d
Cyclospora spp. TMP/SMX PO 5 mg/kg/d and 25
mg/kg/d respectively,
bid 7 d
Blastocystis hominis Metronidazole or iodoquinol Metronidazole PO 30
40 mg/kg/d tid 710 d
Iodoquinol PO 40
mg/kg/d tid 20 d
bid, 2 times a day; EIEC, Enteroinvasive Escherichia coli;EPEC, Enteropathogenic E. coli; ETEC, Enterotoxigenic E. coli; IM,
intramuscular; IV, intravenous; PO, oral; qd, daily; qid, 4 times a day, SMX, sulfamethoxazole; tid, 3 times a day; TMP,
trimethoprim.
Copyright 2008 Elsevier Inc. All rights reserved. - www.mdconsult.com
Page 19 of 19 Chapter 337 - Acute Gastroenteritis in Children from Kliegman: Nelson Textbook o...
1/18/2014 mk:@MSITStore:D:\-%20Documents\+ebook\+pentiing!!!\Nelson%20Text%20Book...
S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Health Benefits of PoulticesDocument7 paginiHealth Benefits of PoulticesEduard50% (2)
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument4 paginiPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralÎncă nu există evaluări
- Introduction To Epidemiology Presented by L. MuparaDocument107 paginiIntroduction To Epidemiology Presented by L. MuparaArwen WellingtonÎncă nu există evaluări
- Trunking CatalogDocument8 paginiTrunking CatalogDenuka PathiranaÎncă nu există evaluări
- Approach To Pleural EffusionDocument46 paginiApproach To Pleural EffusionBaskoro Tri LaksonoÎncă nu există evaluări
- PowerpointDocument29 paginiPowerpointpisces200910Încă nu există evaluări
- Insidious ScreenplayDocument104 paginiInsidious ScreenplayFaisal Hashmi100% (4)
- CHN OutlineDocument5 paginiCHN OutlineMeeKo VideñaÎncă nu există evaluări
- MGR Univ - PerioDocument8 paginiMGR Univ - PerioMohamed FaizalÎncă nu există evaluări
- Oral Lesions and HomoeopathyDocument27 paginiOral Lesions and HomoeopathyDr. Rajneesh Kumar Sharma MD HomÎncă nu există evaluări
- What Is Immunization?Document6 paginiWhat Is Immunization?Aulia RahmawatiÎncă nu există evaluări
- PNEUMONIADocument13 paginiPNEUMONIAshenecajean carajay100% (1)
- Induced SputumDocument6 paginiInduced Sputumnh2411Încă nu există evaluări
- Streptococcus Group A InfectionsDocument13 paginiStreptococcus Group A InfectionsLidia GotoYourhappyplaceÎncă nu există evaluări
- Tropical Health in The Top EndDocument168 paginiTropical Health in The Top Endemkay1234Încă nu există evaluări
- Bonus Task On Politics and GovernanceDocument3 paginiBonus Task On Politics and GovernanceVictorBaguilatÎncă nu există evaluări
- CATARACT Surgery Season Month Wise Reported Figure in IndiaDocument5 paginiCATARACT Surgery Season Month Wise Reported Figure in IndiafriendsofindiaÎncă nu există evaluări
- Descendants - Of.the - Sun.e15.160413.720p 540p 450p XViD WITH IPOP BarosG LIMO CHAOSrel (Viki Version)Document50 paginiDescendants - Of.the - Sun.e15.160413.720p 540p 450p XViD WITH IPOP BarosG LIMO CHAOSrel (Viki Version)MEILINDAÎncă nu există evaluări
- Honolulu Mayor Kirk Caldwell's Letter To Gov. David IgeDocument46 paginiHonolulu Mayor Kirk Caldwell's Letter To Gov. David IgeHonolulu Star-AdvertiserÎncă nu există evaluări
- Approach To An Unconscious PatientDocument62 paginiApproach To An Unconscious Patientangiolikkia80% (5)
- Initial Data Base For Family Nursing Practice: A. Family Structure Characteristics and DynamicsDocument3 paginiInitial Data Base For Family Nursing Practice: A. Family Structure Characteristics and DynamicsjajaÎncă nu există evaluări
- LeprosyDocument22 paginiLeprosyMary Saligan RatoÎncă nu există evaluări
- Intrapartum AssessmentDocument9 paginiIntrapartum AssessmentSarah RiceÎncă nu există evaluări
- Reszon Pi - Typhidot Rapid Igm 2011-01Document2 paginiReszon Pi - Typhidot Rapid Igm 2011-01Harnadi WonogiriÎncă nu există evaluări
- Complications of HemodialysisDocument34 paginiComplications of HemodialysisElza GeorgeÎncă nu există evaluări
- Graduation SpeechDocument3 paginiGraduation SpeechSanseÎncă nu există evaluări
- Final DraftDocument2 paginiFinal Draftapi-444157113Încă nu există evaluări
- Sources of Health Data DraftDocument3 paginiSources of Health Data DraftKarylle PetilÎncă nu există evaluări
- International Health RegulationDocument60 paginiInternational Health RegulationAnonymous 7ugfwjsHQUÎncă nu există evaluări
- Summative TestDocument2 paginiSummative TestmaricelÎncă nu există evaluări