S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Durable Power Attorney FormDocument4 paginiDurable Power Attorney FormRichÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Medication Reconcillation in Home Care Getting Started KitDocument74 paginiMedication Reconcillation in Home Care Getting Started Kitjopet8180Încă nu există evaluări
- Hemodialisis KdoqiDocument183 paginiHemodialisis KdoqiMaFer WueRa100% (2)
- Studer Group Toolkit - HcahpsDocument22 paginiStuder Group Toolkit - Hcahpscervelo_6927100% (2)
- Risk Identification Risk Assessment Plan Risk Response Development Plan Risk Response Control PlanDocument1 paginăRisk Identification Risk Assessment Plan Risk Response Development Plan Risk Response Control PlanEugenio RoweÎncă nu există evaluări
- Brian Racey InformationDocument9 paginiBrian Racey InformationLansdalePatchÎncă nu există evaluări
- Case American Well Group6 PGPUAE2013Document3 paginiCase American Well Group6 PGPUAE2013saurabhpontingÎncă nu există evaluări
- Journal Terapi Dermatitis SeboroikDocument4 paginiJournal Terapi Dermatitis SeboroikMohd Faie RamliÎncă nu există evaluări
- Pharmaceutical Medical Sales Representative in Houston TX Resume Jennifer MillerDocument1 paginăPharmaceutical Medical Sales Representative in Houston TX Resume Jennifer MillerJenniferMiller1Încă nu există evaluări
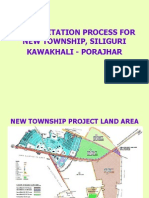
- Presentation On New Township Siliguri 24-11-2011Document29 paginiPresentation On New Township Siliguri 24-11-2011abhijithavalÎncă nu există evaluări
- Titans Fortis N Medi ClinicDocument34 paginiTitans Fortis N Medi ClinicParikshit VermaÎncă nu există evaluări
- PQCNC PFCC Handout 4Document6 paginiPQCNC PFCC Handout 4kcochranÎncă nu există evaluări
- Pricing Reimbursement Drugs In: IndiaDocument28 paginiPricing Reimbursement Drugs In: IndiaGiang HoàngÎncă nu există evaluări
- ABN FormDocument1 paginăABN FormArthur George Jillette JrÎncă nu există evaluări
- 3A - Hospital PharmacyDocument13 pagini3A - Hospital PharmacyekramÎncă nu există evaluări
- Final MCO Working Group ReportDocument77 paginiFinal MCO Working Group ReportShira SchoenbergÎncă nu există evaluări
- NAIC Claim Form PDFDocument3 paginiNAIC Claim Form PDFMohit BaggaÎncă nu există evaluări
- Ajib Diptyanusa - JapanDocument2 paginiAjib Diptyanusa - JapanLorensia Fitra DwitaÎncă nu există evaluări
- CFO Competency Test - AnswersDocument7 paginiCFO Competency Test - AnswersfitzÎncă nu există evaluări
- STAT115 Lecture Notes 1Document4 paginiSTAT115 Lecture Notes 1Jom NicolasÎncă nu există evaluări
- MDCA 1343 Syllabus 2012 16 Weeks-2014-1Document10 paginiMDCA 1343 Syllabus 2012 16 Weeks-2014-1John KellerÎncă nu există evaluări
- Baltimore Afro-American Newspaper, December 25, 2010Document16 paginiBaltimore Afro-American Newspaper, December 25, 2010The AFRO-American NewspapersÎncă nu există evaluări
- Detailed Guilty Verdict For Vernon and Geraldine KlinefelterDocument66 paginiDetailed Guilty Verdict For Vernon and Geraldine KlinefelterDean OlsenÎncă nu există evaluări
- Nursing Home ChargesDocument67 paginiNursing Home Chargesalmond2009Încă nu există evaluări
- Chlorhexidine Gluconate 0.2% W/V Mouth Wash: Class: IndicationsDocument3 paginiChlorhexidine Gluconate 0.2% W/V Mouth Wash: Class: IndicationsAnonymous Bt6favSF4YÎncă nu există evaluări
- Indo UK Health 1000 CR Investment in AmaravatiDocument2 paginiIndo UK Health 1000 CR Investment in AmaravatiVenu VabbilisettyÎncă nu există evaluări
- Evanston Community Assests 02-24-2012Document5 paginiEvanston Community Assests 02-24-2012Ziggy CzykiÎncă nu există evaluări
- 4648 File Birthing Home RequirementsDocument2 pagini4648 File Birthing Home RequirementsnessaÎncă nu există evaluări
- Kola Olatunde Experienced PMDocument3 paginiKola Olatunde Experienced PMRaj MalhotraÎncă nu există evaluări
- Minnesota Property Tax Refund: Forms and InstructionsDocument28 paginiMinnesota Property Tax Refund: Forms and InstructionsJeffery MeyerÎncă nu există evaluări