S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Diversity Added Adaptive-Fuzzy Logic Controlled Receivers For Direct Sequence Code Division Multiple Access SystemDocument10 paginiDiversity Added Adaptive-Fuzzy Logic Controlled Receivers For Direct Sequence Code Division Multiple Access SystemInternational Journal of Emerging Trends in Signal Processing (IJETSP)Încă nu există evaluări
- Advances in QRS Detection: Modified Wavelet Energy Gradient MethodDocument7 paginiAdvances in QRS Detection: Modified Wavelet Energy Gradient MethodInternational Journal of Emerging Trends in Signal Processing (IJETSP)Încă nu există evaluări
- Comparative Study of Various FFT Algorithm Implementation On FPGADocument4 paginiComparative Study of Various FFT Algorithm Implementation On FPGAInternational Journal of Emerging Trends in Signal Processing (IJETSP)Încă nu există evaluări
- Heart Rate Variability Analysis in Iowa Gambling Task: A Glimpse of Patterns Hidden in QRS ComplexDocument8 paginiHeart Rate Variability Analysis in Iowa Gambling Task: A Glimpse of Patterns Hidden in QRS ComplexInternational Journal of Emerging Trends in Signal Processing (IJETSP)Încă nu există evaluări
- Detection of Heart Blocks by Cardiac Cycle Extraction Using Time - Scale AnalysisDocument5 paginiDetection of Heart Blocks by Cardiac Cycle Extraction Using Time - Scale AnalysisInternational Journal of Emerging Trends in Signal Processing (IJETSP)Încă nu există evaluări
- Information Geometry Manifold of Toeplitz Hermitian Positive Definite Covariance Matrices: Mostow/Berger Fibration and Berezin Quantization of Cartan-Siegel DomainsDocument11 paginiInformation Geometry Manifold of Toeplitz Hermitian Positive Definite Covariance Matrices: Mostow/Berger Fibration and Berezin Quantization of Cartan-Siegel DomainsInternational Journal of Emerging Trends in Signal Processing (IJETSP)Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
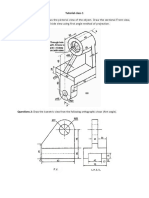
- Tutorial Class 1 Questions 1Document2 paginiTutorial Class 1 Questions 1Bố Quỳnh ChiÎncă nu există evaluări
- Chip DielDocument45 paginiChip DielJUANCANEXTÎncă nu există evaluări
- F4 Search Help To Select More Than One Column ValueDocument4 paginiF4 Search Help To Select More Than One Column ValueRicky DasÎncă nu există evaluări
- TT2223 Week 12a Z-TransformDocument39 paginiTT2223 Week 12a Z-TransformAjiMaulanaÎncă nu există evaluări
- Analysis of Metal Matrix Composite (MMC) Applied Armor System Analysis of Metal Matrix Composite (MMC) Applied Armor SystemDocument8 paginiAnalysis of Metal Matrix Composite (MMC) Applied Armor System Analysis of Metal Matrix Composite (MMC) Applied Armor SystemDerianSyahÎncă nu există evaluări
- Eps Atc 0017 PDFDocument3 paginiEps Atc 0017 PDFSdreamworksÎncă nu există evaluări
- Draft ITP Pipeline Recertification Pearl OILDocument3 paginiDraft ITP Pipeline Recertification Pearl OILIrsyad RosyidiÎncă nu există evaluări
- 1.1 Control Philosophy CAS-1 NMDCDocument36 pagini1.1 Control Philosophy CAS-1 NMDCkoushik42000Încă nu există evaluări
- Microhydro DirectoryDocument4 paginiMicrohydro Directoryrabei romulusÎncă nu există evaluări
- Bloomberg - Transport - SecurityDocument13 paginiBloomberg - Transport - SecurityFernandoÎncă nu există evaluări
- 2x18 AWG Shielded Fire Alarm and Control Cable - 5M11802103Document2 pagini2x18 AWG Shielded Fire Alarm and Control Cable - 5M11802103Alvaro Coy H.Încă nu există evaluări
- Winter Internship Report (23/09/2016 - 31/01/2017)Document56 paginiWinter Internship Report (23/09/2016 - 31/01/2017)AyushÎncă nu există evaluări
- Fire Protection Design For Healthcare FacilitiesDocument34 paginiFire Protection Design For Healthcare Facilitiesapi_fabianÎncă nu există evaluări
- CTLG MINI08engDocument48 paginiCTLG MINI08enggadacz111Încă nu există evaluări
- Course Material Fees: Terms 1190 - 1193Document8 paginiCourse Material Fees: Terms 1190 - 1193Frances Ijeoma ObiakorÎncă nu există evaluări
- Programmable Safety Systems PSS-Range: Service Tool PSS SW QLD, From Version 4.2 Operating Manual Item No. 19 461Document18 paginiProgrammable Safety Systems PSS-Range: Service Tool PSS SW QLD, From Version 4.2 Operating Manual Item No. 19 461MAICK_ITSÎncă nu există evaluări
- Draft BLDocument3 paginiDraft BLimam faodjiÎncă nu există evaluări
- En 12604 (2000) (E)Document7 paginiEn 12604 (2000) (E)Carlos LanzillottoÎncă nu există evaluări
- Computer SoftwareDocument3 paginiComputer SoftwareCyrine CalagosÎncă nu există evaluări
- Metric DIN 434 Square Taper Washers: Visit Our For Product AvailabilityDocument4 paginiMetric DIN 434 Square Taper Washers: Visit Our For Product AvailabilityRodrigoÎncă nu există evaluări
- Fasteners Lecture 11-20-03Document67 paginiFasteners Lecture 11-20-03laponggaÎncă nu există evaluări
- Circuito PCB Control Pedal V3 TerminadoDocument1 paginăCircuito PCB Control Pedal V3 TerminadoMarcelo PereiraÎncă nu există evaluări
- Drying AgentDocument36 paginiDrying AgentSo MayeÎncă nu există evaluări
- Manual Construction Standards Completo CorregidozDocument240 paginiManual Construction Standards Completo CorregidozJose DiazÎncă nu există evaluări
- PDK Repair Aftersales TrainingDocument22 paginiPDK Repair Aftersales TrainingEderson BJJÎncă nu există evaluări
- CHE 322 - Gaseous Fuel ProblemsDocument26 paginiCHE 322 - Gaseous Fuel ProblemsDanice LunaÎncă nu există evaluări
- Tailless AircraftDocument17 paginiTailless AircraftVikasVickyÎncă nu există evaluări
- SW Product SummaryDocument64 paginiSW Product SummaryFabio MenegatoÎncă nu există evaluări
- An Overview of Subspace Identification: S. Joe QinDocument12 paginiAn Overview of Subspace Identification: S. Joe QinGodofredoÎncă nu există evaluări
- Seamless Fiux Fored Wire - Megafil250Document1 paginăSeamless Fiux Fored Wire - Megafil250SungJun ParkÎncă nu există evaluări