S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Tomorrow Is WaitingDocument8 paginiTomorrow Is WaitingsrplsmskÎncă nu există evaluări
- Outline PatentsDocument37 paginiOutline Patentspbp613Încă nu există evaluări
- Harsha Akka 013759 Unit 13 CRP Report PDFDocument94 paginiHarsha Akka 013759 Unit 13 CRP Report PDFMinda RajanÎncă nu există evaluări
- Global Davit GMBHDocument8 paginiGlobal Davit GMBHTimothy JacksonÎncă nu există evaluări
- 10 Must Read Books For Stock Market Investors in India - Trade BrainsDocument35 pagini10 Must Read Books For Stock Market Investors in India - Trade BrainsCHANDRAKISHORE SINGHÎncă nu există evaluări
- Architecture As SpaceDocument31 paginiArchitecture As Spaceazimkhtr50% (4)
- AVSEC Awareness Ground StaffDocument12 paginiAVSEC Awareness Ground Staffanon_823464996100% (2)
- Air AbrasionDocument9 paginiAir AbrasionbarcimÎncă nu există evaluări
- Cuspal Deflection and Microleakage in Premolar Teeth Restored With Bulk-Fill Flowable Resin-Based Composite Base MaterialsDocument27 paginiCuspal Deflection and Microleakage in Premolar Teeth Restored With Bulk-Fill Flowable Resin-Based Composite Base MaterialsbarcimÎncă nu există evaluări
- Endodontic Diagnosis/Pulp Tests and Etiology of Pulp InflammationDocument3 paginiEndodontic Diagnosis/Pulp Tests and Etiology of Pulp InflammationbarcimÎncă nu există evaluări
- Priyanka Arien Dr.Document5 paginiPriyanka Arien Dr.barcimÎncă nu există evaluări
- Regenerative Endodontic Treatment (Revascularization)Document4 paginiRegenerative Endodontic Treatment (Revascularization)barcimÎncă nu există evaluări
- Long-Term Dentoskeletal Effects and Facial Profile Changes Induced by Bionator TherapyDocument8 paginiLong-Term Dentoskeletal Effects and Facial Profile Changes Induced by Bionator TherapybarcimÎncă nu există evaluări
- Stability Evaluation of Occlusal Changes Obtained With Fränkel's Function Regulator-2Document8 paginiStability Evaluation of Occlusal Changes Obtained With Fränkel's Function Regulator-2barcimÎncă nu există evaluări
- Xerostomia in Patients On Chronic Hemodialysis. Nat Rev Nephrol 8:176-182Document8 paginiXerostomia in Patients On Chronic Hemodialysis. Nat Rev Nephrol 8:176-182barcimÎncă nu există evaluări
- Saddle LapDocument7 paginiSaddle LapbarcimÎncă nu există evaluări
- Clinical Effects of Removable Functional Twin Block Appliance in The Treatment of Class Ii/1 MalocclusionDocument6 paginiClinical Effects of Removable Functional Twin Block Appliance in The Treatment of Class Ii/1 MalocclusionbarcimÎncă nu există evaluări
- Association of MSX1 and TGFB3 With Nonsyndromic Clefting in HumansDocument12 paginiAssociation of MSX1 and TGFB3 With Nonsyndromic Clefting in HumansbarcimÎncă nu există evaluări
- 10 FullDocument12 pagini10 FullbarcimÎncă nu există evaluări
- 1 Case ReportDocument3 pagini1 Case ReportbarcimÎncă nu există evaluări
- Article-PDF-baljeet Singh Puneet Bajaj Grunam Singh-141Document3 paginiArticle-PDF-baljeet Singh Puneet Bajaj Grunam Singh-141barcimÎncă nu există evaluări
- Saliva As A Diagnostic Fluid: Salivary Glands and Saliva Number 3Document8 paginiSaliva As A Diagnostic Fluid: Salivary Glands and Saliva Number 3barcimÎncă nu există evaluări
- Periodontitis and Semm Lnterleukin-6 Levels in The ElderlyDocument3 paginiPeriodontitis and Semm Lnterleukin-6 Levels in The ElderlybarcimÎncă nu există evaluări
- Sample Cover LetterDocument6 paginiSample Cover LettermohitÎncă nu există evaluări
- Pe Unit Plan TemplateDocument3 paginiPe Unit Plan Templateapi-239320998Încă nu există evaluări
- Dictum Giftideas 2012Document40 paginiDictum Giftideas 2012Alexandre LetellierÎncă nu există evaluări
- (Myers79) (Hetzel88)Document43 pagini(Myers79) (Hetzel88)Infomailbox10Încă nu există evaluări
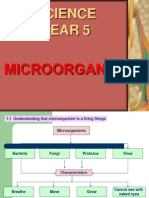
- Science Year 5: MicroorganismsDocument8 paginiScience Year 5: MicroorganismscthanifahÎncă nu există evaluări
- 2000 - VAICTM-an Accounting Tool For IC Management - Ante PulicDocument13 pagini2000 - VAICTM-an Accounting Tool For IC Management - Ante PulicIklima RahmaÎncă nu există evaluări
- SikaWrap®-900 CDocument4 paginiSikaWrap®-900 CN.J. PatelÎncă nu există evaluări
- Qualities of Effective Business LettersDocument39 paginiQualities of Effective Business Letterskrystel0% (1)
- Ethics and Social Responsibilities of Entrepreneurship PDFDocument4 paginiEthics and Social Responsibilities of Entrepreneurship PDFRevuru ArunaÎncă nu există evaluări
- LKPD Bahasa Inggris Kelas VII - Descriptive TextDocument1 paginăLKPD Bahasa Inggris Kelas VII - Descriptive TextAhmad Farel HusainÎncă nu există evaluări
- Lecture 9Document26 paginiLecture 9Tesfaye ejetaÎncă nu există evaluări
- Cable Subjected To Concentrated Loads CaDocument41 paginiCable Subjected To Concentrated Loads CaIcy MakerÎncă nu există evaluări
- MBA: International Business: SchillerDocument2 paginiMBA: International Business: SchillernancyekkaÎncă nu există evaluări
- Abaqus Example Using Beam ElementsDocument18 paginiAbaqus Example Using Beam ElementsŞener KılıçÎncă nu există evaluări
- CEFR Lesson Plan Let's PlayDocument1 paginăCEFR Lesson Plan Let's PlayRashidah Zaman100% (3)
- Вправи на Past SimpleDocument4 paginiВправи на Past SimpleLiliaÎncă nu există evaluări
- 13-25-551 - 08 - 120121 Compresor Gardern DenverDocument102 pagini13-25-551 - 08 - 120121 Compresor Gardern DenverArleyTrujillo1224Încă nu există evaluări
- 3 ReviewsDocument14 pagini3 ReviewsGabriela ZambranoÎncă nu există evaluări
- Hyperbolic FunctionsDocument11 paginiHyperbolic FunctionsShiraz NajatÎncă nu există evaluări
- WAP Push and MMS For Android Rev6Document4 paginiWAP Push and MMS For Android Rev6Shruti MahadikÎncă nu există evaluări
- Lesson Plan Template 2017 7 3Document4 paginiLesson Plan Template 2017 7 3api-424474395Încă nu există evaluări
- Lino PresentationDocument14 paginiLino Presentationapi-356807903Încă nu există evaluări
- In The Star Schema DesignDocument11 paginiIn The Star Schema DesignppavandsÎncă nu există evaluări