S-ar putea să vă placă și
- MDT World Press Newsletter Full PDF Vol2No3Document19 paginiMDT World Press Newsletter Full PDF Vol2No3Alexandra NadinneÎncă nu există evaluări
- Impact Factor 2016Document233 paginiImpact Factor 2016Alexandra NadinneÎncă nu există evaluări
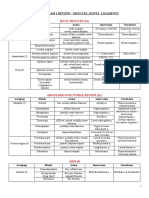
- Anatomy Exam 1 Review - Muscles of the Back, Shoulder, Arm, Forearm & HandDocument27 paginiAnatomy Exam 1 Review - Muscles of the Back, Shoulder, Arm, Forearm & Handgdubs215Încă nu există evaluări
- Muscle Origin Insertion ActionsDocument14 paginiMuscle Origin Insertion ActionsAlexandra NadinneÎncă nu există evaluări
- A Statistical Architecture For Economic Statistics: Ron Mckenzie Ices IiiDocument34 paginiA Statistical Architecture For Economic Statistics: Ron Mckenzie Ices IiiRishikesh KaushikÎncă nu există evaluări
- Chartered Society of Physiotherapy Uk and Countries March 2017 v1Document16 paginiChartered Society of Physiotherapy Uk and Countries March 2017 v1Alexandra NadinneÎncă nu există evaluări
- Bio EnergeticsDocument23 paginiBio EnergeticsAlexandra NadinneÎncă nu există evaluări
- 13 CIN Respiratory Assessment NotesDocument29 pagini13 CIN Respiratory Assessment NotesAlexandra NadinneÎncă nu există evaluări
- Bers Resp No Anim 03Document65 paginiBers Resp No Anim 03Alexandra NadinneÎncă nu există evaluări
- Behavior and MedicineDocument32 paginiBehavior and MedicineAlexandra NadinneÎncă nu există evaluări
- Egeszsegugyi Ellatas Fuzet EngDocument16 paginiEgeszsegugyi Ellatas Fuzet EngAlexandra NadinneÎncă nu există evaluări
- Phy Kompetenzprofil Englisch Fin 02106Document22 paginiPhy Kompetenzprofil Englisch Fin 02106Alexandra NadinneÎncă nu există evaluări
- Patients' Rights in the European Union OverviewDocument30 paginiPatients' Rights in the European Union OverviewAlexandra NadinneÎncă nu există evaluări
- Health Services Co108 enDocument11 paginiHealth Services Co108 enAlexandra NadinneÎncă nu există evaluări
- c1Document7 paginic1Alexandra NadinneÎncă nu există evaluări
- 2012-2173 Physical Agent Catalog - 2Document16 pagini2012-2173 Physical Agent Catalog - 2Alexandra NadinneÎncă nu există evaluări
- Icahe Oc Incontinence User ManualDocument118 paginiIcahe Oc Incontinence User ManualAlexandra NadinneÎncă nu există evaluări
- 1 s2.0 S0004951408700072 MainDocument5 pagini1 s2.0 S0004951408700072 MainAlexandra NadinneÎncă nu există evaluări
- Electrotherapy For Neck Pain (Review)Document106 paginiElectrotherapy For Neck Pain (Review)Alexandra NadinneÎncă nu există evaluări
- Evidence Informed Practice Position Statement EnglishDocument2 paginiEvidence Informed Practice Position Statement EnglishAlexandra NadinneÎncă nu există evaluări
- Clinical Data Fisiotek HP2Document28 paginiClinical Data Fisiotek HP2Alexandra NadinneÎncă nu există evaluări
- Colleague and Patient Questionnaires - PDF 44702599Document12 paginiColleague and Patient Questionnaires - PDF 44702599Alexandra NadinneÎncă nu există evaluări
- 1 s2.0 S0004951408700072 MainDocument5 pagini1 s2.0 S0004951408700072 MainAlexandra NadinneÎncă nu există evaluări
- Nu e Nimic InteresantDocument10 paginiNu e Nimic InteresantAlexandra NadinneÎncă nu există evaluări
- The Physiotherapy Workforce Is Ageing, Becoming More Masculinised, and Is Working Longer Hours: A Demographic StudyDocument6 paginiThe Physiotherapy Workforce Is Ageing, Becoming More Masculinised, and Is Working Longer Hours: A Demographic StudyAlexandra NadinneÎncă nu există evaluări
- Should I: Warn The Patient First?Document7 paginiShould I: Warn The Patient First?Alexandra NadinneÎncă nu există evaluări
- Un Peu Du Ethics Pour RehabilitationDocument8 paginiUn Peu Du Ethics Pour RehabilitationAlexandra NadinneÎncă nu există evaluări
- 02 Leveraging Employee Engagement For Competitive Advantage 2Document12 pagini02 Leveraging Employee Engagement For Competitive Advantage 2faisalsiddique100% (2)
- J Hist Med Allied Sci 2005 Linker 320 54Document35 paginiJ Hist Med Allied Sci 2005 Linker 320 54Alexandra NadinneÎncă nu există evaluări
- Scheda I-Tech Ue - Eng (Sp21-00)Document2 paginiScheda I-Tech Ue - Eng (Sp21-00)Alexandra NadinneÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Priyanka ProjectDocument30 paginiPriyanka ProjectPriyanka ValluriÎncă nu există evaluări
- How manual therapy concepts have evolved from original researchDocument6 paginiHow manual therapy concepts have evolved from original researchismaelvara6568Încă nu există evaluări
- Nursing Care For Patients With Musculoskeletal DisordersDocument4 paginiNursing Care For Patients With Musculoskeletal DisordersMark Russel Sean LealÎncă nu există evaluări
- Lec 12 - Drugs Used in PTDocument14 paginiLec 12 - Drugs Used in PTAiqa QaziÎncă nu există evaluări
- Association between acute low back pain and fear of movementDocument5 paginiAssociation between acute low back pain and fear of movementRadhamani ArunÎncă nu există evaluări
- TX Hospital Licensing Rules Table of ContentsDocument318 paginiTX Hospital Licensing Rules Table of ContentskazooedÎncă nu există evaluări
- WT-Natasha Dobby TEXTDocument4 paginiWT-Natasha Dobby TEXTjisha tom100% (3)
- NP 5Document6 paginiNP 5Ana Blesilda Cachola100% (1)
- Active Rehab for Back, Neck, Shoulder PainDocument57 paginiActive Rehab for Back, Neck, Shoulder PainLindawatiAjaÎncă nu există evaluări
- Bubble Wrap Gross Motor Skills ActivitiesDocument3 paginiBubble Wrap Gross Motor Skills ActivitiesNoreen GriffinÎncă nu există evaluări
- Physiotherapy Management of Acute Transverse Myelitis in A Pediatric Patient in A Nigerian Hospital: A Case ReportDocument9 paginiPhysiotherapy Management of Acute Transverse Myelitis in A Pediatric Patient in A Nigerian Hospital: A Case Reportluis bulnesÎncă nu există evaluări
- Guidelines For Data Collection On The American Nurses Association's National Quality Forum Endorsed MeasuresDocument21 paginiGuidelines For Data Collection On The American Nurses Association's National Quality Forum Endorsed MeasuresMaria Fudji HastutiÎncă nu există evaluări
- Multiple Choice RatioDocument14 paginiMultiple Choice RatioDivine Joe Grace Marcelino100% (2)
- The Movement Continuum Theory of Physical Therapy-2Document2 paginiThe Movement Continuum Theory of Physical Therapy-2Ingela Sjölin100% (2)
- Certificate of DisabiltyDocument2 paginiCertificate of DisabiltyRizwan KhanÎncă nu există evaluări
- Documentation For Physical Therapist Assistants by Wendy D. Bircher Wendy D. BircherDocument304 paginiDocumentation For Physical Therapist Assistants by Wendy D. Bircher Wendy D. BircherRickDÎncă nu există evaluări
- Recommendations For Physiotherapy Intervention After Stroke 5712Document9 paginiRecommendations For Physiotherapy Intervention After Stroke 5712Anonymous Ezsgg0VSEÎncă nu există evaluări
- EXSA - Silver Award Recipients 2007Document8 paginiEXSA - Silver Award Recipients 2007applebarrelÎncă nu există evaluări
- Document PDFDocument12 paginiDocument PDFEviÎncă nu există evaluări
- Business & Marketing PortfolioDocument28 paginiBusiness & Marketing PortfolioByng Sumague100% (3)
- Deborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDocument5 paginiDeborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDago Angel Prieto PalavecinoÎncă nu există evaluări
- Jessica Irwin Resume 2020 RNDocument2 paginiJessica Irwin Resume 2020 RNapi-300943374Încă nu există evaluări
- Process of Rehabilitation in PsychiatryDocument29 paginiProcess of Rehabilitation in PsychiatryRahul Kumar DiwakarÎncă nu există evaluări
- Aquatic Therapy Journal Aug 2005 Vol 7Document28 paginiAquatic Therapy Journal Aug 2005 Vol 7Barbu Alexandru StefanÎncă nu există evaluări
- Superior Outcomes After Operative Fixation of Patella Fractures Using A Novel Plating Technique - A Prospective Cohort StudyDocument25 paginiSuperior Outcomes After Operative Fixation of Patella Fractures Using A Novel Plating Technique - A Prospective Cohort StudyAldrovando JrÎncă nu există evaluări
- In Another CountryDocument10 paginiIn Another CountryHồng NhungÎncă nu există evaluări
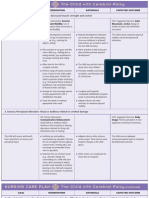
- Nursing Care Plan Goals for Child with Cerebral PalsyDocument3 paginiNursing Care Plan Goals for Child with Cerebral PalsyJamie Icabandi67% (3)
- Cambridge International Advanced Subsidiary and Advanced LevelDocument4 paginiCambridge International Advanced Subsidiary and Advanced LevelAdelina AÎncă nu există evaluări
- Medical Rehabilitation Exercises Improve Joints MusclesDocument5 paginiMedical Rehabilitation Exercises Improve Joints MusclessylviaÎncă nu există evaluări
- Doors Pages From VA ARCH DESIGN MANUALDocument13 paginiDoors Pages From VA ARCH DESIGN MANUALMic BÎncă nu există evaluări