S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Current ChargesDocument1 paginăCurrent ChargesMajkel Benche Custodio MllÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Move in Notice PDFDocument1 paginăMove in Notice PDFMajkel Benche Custodio MllÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Affiliate Launch Strategy DRAFT For QuickProDocument6 paginiAffiliate Launch Strategy DRAFT For QuickProMajkel Benche Custodio MllÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- PLDT Application 18R Marco PoloDocument1 paginăPLDT Application 18R Marco PoloMajkel Benche Custodio MllÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- QuickPro Affiliate System Development Proposal 07.6.22Document7 paginiQuickPro Affiliate System Development Proposal 07.6.22Majkel Benche Custodio MllÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Freelancer ContractDocument4 paginiFreelancer ContractMajkel Benche Custodio Mll50% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- DX DiagDocument30 paginiDX DiagMajkel Benche Custodio MllÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Sales Receipt: Date Activity Description QTY Rate AmountDocument1 paginăSales Receipt: Date Activity Description QTY Rate AmountMajkel Benche Custodio MllÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- How To Create A ResumeDocument2 paginiHow To Create A ResumeMajkel Benche Custodio Mll100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Thank You For Your Purchase: Click Here TO Get Your Eboo KDocument1 paginăThank You For Your Purchase: Click Here TO Get Your Eboo KMajkel Benche Custodio MllÎncă nu există evaluări
- Cebu City Sda Church Voice of Youth CrusadeDocument1 paginăCebu City Sda Church Voice of Youth CrusadeMajkel Benche Custodio MllÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Maj IntroDocument2 paginiMaj IntroMajkel Benche Custodio MllÎncă nu există evaluări
- Resumed KST 0918Document1 paginăResumed KST 0918Majkel Benche Custodio MllÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- 4th Auguest 2016 Fluid and Hemodynamic Disorders 2011Document81 pagini4th Auguest 2016 Fluid and Hemodynamic Disorders 2011Majkel Benche Custodio MllÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Fijabi Ireoluwa: Risk Factors of Chronic BronchitisDocument4 paginiFijabi Ireoluwa: Risk Factors of Chronic BronchitisMajkel Benche Custodio MllÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- In The Cross - Worthy Is The Lamb - Crown Him With Many Crowns SATB10L - P PianoDocument6 paginiIn The Cross - Worthy Is The Lamb - Crown Him With Many Crowns SATB10L - P PianoMajkel Benche Custodio MllÎncă nu există evaluări
- Anti-Oxidant Properties of Goose Grass: BibliographyDocument2 paginiAnti-Oxidant Properties of Goose Grass: BibliographyMajkel Benche Custodio MllÎncă nu există evaluări
- Icu ApDocument1 paginăIcu ApMajkel Benche Custodio MllÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Hugas Plato Prepare Lunch: Cleanliness Is Next To GodlinessDocument2 paginiHugas Plato Prepare Lunch: Cleanliness Is Next To GodlinessMajkel Benche Custodio MllÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
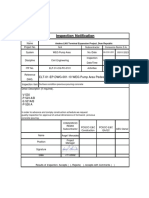
- In-CIV-201 INSPECTION NOTIFICATION Pre-Pouring Concrete WEG Pump Area PedestalsDocument5 paginiIn-CIV-201 INSPECTION NOTIFICATION Pre-Pouring Concrete WEG Pump Area PedestalsPedro PaulinoÎncă nu există evaluări
- Sop Draft Utas Final-2Document4 paginiSop Draft Utas Final-2Himanshu Waster0% (1)
- Tally Trading and Profit Loss Acc Balance SheetDocument14 paginiTally Trading and Profit Loss Acc Balance Sheetsuresh kumar10Încă nu există evaluări
- Adobe Scan 03-May-2021Document22 paginiAdobe Scan 03-May-2021Mohit RanaÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- NZAA ChartsDocument69 paginiNZAA ChartsA340_600100% (5)
- 6 Chase Nat'l Bank of New York V BattatDocument2 pagini6 Chase Nat'l Bank of New York V BattatrÎncă nu există evaluări
- Italian Budgeting Policy Between Punctuations and Incrementalism Alice Cavalieri Full ChapterDocument51 paginiItalian Budgeting Policy Between Punctuations and Incrementalism Alice Cavalieri Full Chapterjames.philson408Încă nu există evaluări
- GDPR Whitepaper FormsDocument13 paginiGDPR Whitepaper FormsRui Cruz100% (6)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Ekotoksikologi Kelautan PDFDocument18 paginiEkotoksikologi Kelautan PDFMardia AlwanÎncă nu există evaluări
- Trifles Summary and Analysis of Part IDocument11 paginiTrifles Summary and Analysis of Part IJohn SmytheÎncă nu există evaluări
- Literacy Technology of The IntellectDocument20 paginiLiteracy Technology of The IntellectFrances Tay100% (1)
- Tail Lamp Left PDFDocument1 paginăTail Lamp Left PDFFrancis RodrigueÎncă nu există evaluări
- MAKAUT CIVIL Syllabus SEM 8Document9 paginiMAKAUT CIVIL Syllabus SEM 8u9830120786Încă nu există evaluări
- Cuthites: Cuthites in Jewish LiteratureDocument2 paginiCuthites: Cuthites in Jewish LiteratureErdincÎncă nu există evaluări
- Philippine Politics and Governance: Lesson 6: Executive DepartmentDocument24 paginiPhilippine Politics and Governance: Lesson 6: Executive DepartmentAndrea IbañezÎncă nu există evaluări
- Resume-Pam NiehoffDocument2 paginiResume-Pam Niehoffapi-253710681Încă nu există evaluări
- "Working Capital Management": Master of CommerceDocument4 pagini"Working Capital Management": Master of Commercekunal bankheleÎncă nu există evaluări
- Remote Lab 1013Document3 paginiRemote Lab 1013cloud scapeÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Sailpoint Training Understanding ReportDocument2 paginiSailpoint Training Understanding ReportKunalGuptaÎncă nu există evaluări
- DLF New Town Gurgaon Soicety Handbook RulesDocument38 paginiDLF New Town Gurgaon Soicety Handbook RulesShakespeareWallaÎncă nu există evaluări
- WT WIAB Reworked CH 3 FullDocument5 paginiWT WIAB Reworked CH 3 Fulljack3314sonyÎncă nu există evaluări
- GR - 211015 - 2016 Cepalco Vs Cepalco UnionDocument14 paginiGR - 211015 - 2016 Cepalco Vs Cepalco UnionHenteLAWcoÎncă nu există evaluări
- Definition of Social PharmacyDocument7 paginiDefinition of Social PharmacyShraddha PharmacyÎncă nu există evaluări
- Shop Decjuba White DressDocument1 paginăShop Decjuba White DresslovelyÎncă nu există evaluări
- CT 1 - QP - Icse - X - GSTDocument2 paginiCT 1 - QP - Icse - X - GSTAnanya IyerÎncă nu există evaluări
- MPERSDocument1 paginăMPERSKen ChiaÎncă nu există evaluări
- Lean Supply Chains: Chapter FourteenDocument29 paginiLean Supply Chains: Chapter FourteenKshitij SharmaÎncă nu există evaluări
- Rakesh Ali: Centre Manager (Edubridge Learning Pvt. LTD)Document2 paginiRakesh Ali: Centre Manager (Edubridge Learning Pvt. LTD)HRD CORP CONSULTANCYÎncă nu există evaluări
- MC Script For StorytellingDocument1 paginăMC Script For StorytellingPPD LUBOK ANTU-CM15 KPMÎncă nu există evaluări
- Nuclear Power Plants PDFDocument64 paginiNuclear Power Plants PDFmvlxlxÎncă nu există evaluări
- Magnolia Table, Volume 3: A Collection of Recipes for GatheringDe la EverandMagnolia Table, Volume 3: A Collection of Recipes for GatheringEvaluare: 4.5 din 5 stele4.5/5 (4)
- The Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayDe la EverandThe Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayÎncă nu există evaluări
- Mostly Plants: 101 Delicious Flexitarian Recipes from the Pollan FamilyDe la EverandMostly Plants: 101 Delicious Flexitarian Recipes from the Pollan FamilyEvaluare: 4 din 5 stele4/5 (11)