S-ar putea să vă placă și
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsDe la EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsEvaluare: 5 din 5 stele5/5 (9)
- Clinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3De la EverandClinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3Evaluare: 5 din 5 stele5/5 (1)
- Paediatric Dosage of Some Drugs-1Document45 paginiPaediatric Dosage of Some Drugs-1JaneÎncă nu există evaluări
- JCI Infographic IPSGDocument1 paginăJCI Infographic IPSGwoouuw0903100% (1)
- Artemisinin in Cancer Treatment - SinghDocument29 paginiArtemisinin in Cancer Treatment - SinghLaa Lalaa100% (1)
- Pedia 3.2 - IMCI (Vision) PDFDocument14 paginiPedia 3.2 - IMCI (Vision) PDFKaren ValdezÎncă nu există evaluări
- Routine Antenatal Screening DR - Amy MellorDocument3 paginiRoutine Antenatal Screening DR - Amy MellorYwagar Ywagar100% (1)
- Adverse Effects of Falciparum and Vivax Malaria and The Safety of Antimalarial Treatment in Early Pregnancy - A Population-Based StudyDocument9 paginiAdverse Effects of Falciparum and Vivax Malaria and The Safety of Antimalarial Treatment in Early Pregnancy - A Population-Based StudyPerdana SamektoÎncă nu există evaluări
- Antenatal Betamethasone For Women at RiskDocument10 paginiAntenatal Betamethasone For Women at RiskThapakorn JalearnyingÎncă nu există evaluări
- 2015 Article 794Document9 pagini2015 Article 794Hyung ArdiÎncă nu există evaluări
- Wiktor 1999. MTCT Cote DIvoire.Document5 paginiWiktor 1999. MTCT Cote DIvoire.alemd23Încă nu există evaluări
- Oracle IDocument10 paginiOracle Imaxis4xÎncă nu există evaluări
- 2012 Article 61Document5 pagini2012 Article 61Al MubartaÎncă nu există evaluări
- Jir 558Document7 paginiJir 558Hyung ArdiÎncă nu există evaluări
- MorbiliDocument7 paginiMorbilijourey08Încă nu există evaluări
- 140 140 1 PBDocument4 pagini140 140 1 PBMina LelymanÎncă nu există evaluări
- New England Journal Medicine: The ofDocument11 paginiNew England Journal Medicine: The ofDevina Indah PermatasariÎncă nu există evaluări
- Progesterone and The Risk of Preterm Birth Among Women With A Short CervixDocument8 paginiProgesterone and The Risk of Preterm Birth Among Women With A Short Cervixangela_karenina_1Încă nu există evaluări
- Expectant Versus Aggressive Management in Severe Preeclampsia Remote From TermDocument6 paginiExpectant Versus Aggressive Management in Severe Preeclampsia Remote From Termmiss.JEJEÎncă nu există evaluări
- Afhs0801 0044 2Document6 paginiAfhs0801 0044 2Noval FarlanÎncă nu există evaluări
- Medical Record Validation of Maternally Reported History of PreeclampsiDocument7 paginiMedical Record Validation of Maternally Reported History of PreeclampsiezaÎncă nu există evaluări
- J of Obstet and Gynaecol - 2012 - Aksornphusitaphong - Risk Factors of Early and Late Onset Pre EclampsiaDocument5 paginiJ of Obstet and Gynaecol - 2012 - Aksornphusitaphong - Risk Factors of Early and Late Onset Pre EclampsiaDefi SelvianitaÎncă nu există evaluări
- A Prospective Cohort Study of Pregnancy Risk Factors and Birth Outcomes in Aboriginal WomenDocument5 paginiA Prospective Cohort Study of Pregnancy Risk Factors and Birth Outcomes in Aboriginal WomenFirman DariyansyahÎncă nu există evaluări
- Roush An 2011Document3 paginiRoush An 2011hamadahutpÎncă nu există evaluări
- Nej Mo A 0807381Document12 paginiNej Mo A 0807381Mildred MontÎncă nu există evaluări
- Konstantopoulos 2020Document14 paginiKonstantopoulos 2020Corey WoodsÎncă nu există evaluări
- Nejmoa 1310214Document11 paginiNejmoa 1310214Aura RachmawatiÎncă nu există evaluări
- NEONATAL MALARIA New OneDocument41 paginiNEONATAL MALARIA New Onemufracaca60% (5)
- Induction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationDocument6 paginiInduction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationFebrinata MahadikaÎncă nu există evaluări
- Jurnal GiziDocument7 paginiJurnal GizijuwitapratiwiÎncă nu există evaluări
- Aggressive Intervention of Previable Preterm Premature Rupture of MembranesDocument8 paginiAggressive Intervention of Previable Preterm Premature Rupture of MembranesVanessa Riaño GodoyÎncă nu există evaluări
- Scopus (29) Many2017Document7 paginiScopus (29) Many2017ika puspitaÎncă nu există evaluări
- Mifepristone and Misoprostol For Early Pregnancy Failure: A Cohort AnalysisDocument6 paginiMifepristone and Misoprostol For Early Pregnancy Failure: A Cohort AnalysisBobby SetiawanÎncă nu există evaluări
- Enoxaparin and AspirinDocument11 paginiEnoxaparin and AspirinFemtom PriyoÎncă nu există evaluări
- Treatment of Asymptomatic Vaginal Candidiasis in Pregnancy To Prevent Preterm Birth An Openlabel Pilot Randomized ContrDocument7 paginiTreatment of Asymptomatic Vaginal Candidiasis in Pregnancy To Prevent Preterm Birth An Openlabel Pilot Randomized ContrariestianiÎncă nu există evaluări
- 1 s2.0 S1110569015300042 MainDocument5 pagini1 s2.0 S1110569015300042 MainAzam alausyÎncă nu există evaluări
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 paginiAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniÎncă nu există evaluări
- BMC Pediatrics PregnancyDocument8 paginiBMC Pediatrics PregnancyMobin Ur Rehman KhanÎncă nu există evaluări
- ANESTHESIOLOGY (R) 2016 - Refresher Course Lecture Summaries副本(被拖移)Document9 paginiANESTHESIOLOGY (R) 2016 - Refresher Course Lecture Summaries副本(被拖移)Han biaoÎncă nu există evaluări
- 33873-Article Text-121761-1-10-20170831Document6 pagini33873-Article Text-121761-1-10-20170831AnggaÎncă nu există evaluări
- Jurnal AsliDocument5 paginiJurnal Aslipramono hanumÎncă nu există evaluări
- Acute Pyelonephritis in PregnancyDocument7 paginiAcute Pyelonephritis in PregnancyKvmLlyÎncă nu există evaluări
- Omj D 09 00101Document6 paginiOmj D 09 00101DewinsÎncă nu există evaluări
- Omega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenDocument10 paginiOmega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenJojo RyelciusÎncă nu există evaluări
- Pre-Eclampsia, Eclampsia and Adverse Maternal and Perinatal Outcomes: A Secondary Analysis of The World Health Organization Multicountry Survey On Maternal and Newborn HealthDocument11 paginiPre-Eclampsia, Eclampsia and Adverse Maternal and Perinatal Outcomes: A Secondary Analysis of The World Health Organization Multicountry Survey On Maternal and Newborn HealthMariana CruzÎncă nu există evaluări
- Article 233230Document11 paginiArticle 233230arreyemilieneÎncă nu există evaluări
- Nejm 2020 1908380Document31 paginiNejm 2020 1908380Dhruvi KansaraÎncă nu există evaluări
- Malaria Journal Malaria JournalDocument20 paginiMalaria Journal Malaria JournalYuda Arie DharmawanÎncă nu există evaluări
- Asymptomatic Trichomonas and Candida Colonization and Pregnancy OutcomeDocument7 paginiAsymptomatic Trichomonas and Candida Colonization and Pregnancy OutcomealvilÎncă nu există evaluări
- Case Report: Multidrug-Resistant Tuberculosis During Pregnancy: Two Case Reports and Review of The LiteratureDocument4 paginiCase Report: Multidrug-Resistant Tuberculosis During Pregnancy: Two Case Reports and Review of The Literaturesyarifah ghina basirohÎncă nu există evaluări
- Sabai 2000Document6 paginiSabai 2000Min ThuÎncă nu există evaluări
- Determinants of Pre-Eclampsia Incidence Among Pregnant Women in Antenatal Care at Fortportal Regional Referral HospitalDocument14 paginiDeterminants of Pre-Eclampsia Incidence Among Pregnant Women in Antenatal Care at Fortportal Regional Referral HospitalKIU PUBLICATION AND EXTENSIONÎncă nu există evaluări
- Jurnal Analisis 2 Uts Mikrobiologi Dan ParasitologiDocument10 paginiJurnal Analisis 2 Uts Mikrobiologi Dan ParasitologipujiÎncă nu există evaluări
- Diagnosis Treatment MalariaDocument29 paginiDiagnosis Treatment MalariaAnuradha Akolekar-mahadik100% (1)
- Malaria in Pregnancy A Literature Review JournalDocument4 paginiMalaria in Pregnancy A Literature Review Journalc5p0cd99100% (1)
- Maternal and Perinatal Complications of Severe Preeclampsia in Three Referral Hospitals in Yaoundé, CameroonDocument8 paginiMaternal and Perinatal Complications of Severe Preeclampsia in Three Referral Hospitals in Yaoundé, CameroonIke Istofani KÎncă nu există evaluări
- Original ArticleDocument4 paginiOriginal ArticlefeyzarezarÎncă nu există evaluări
- Prevalence of Abnormal Pap Smear During Pregnancy in A Teaching Hospital in South IndiaDocument4 paginiPrevalence of Abnormal Pap Smear During Pregnancy in A Teaching Hospital in South IndiapebripulunganÎncă nu există evaluări
- Brmedj00008 0063cDocument1 paginăBrmedj00008 0063cNahrisyah Ulfa SafnaÎncă nu există evaluări
- Piis0002937811009185 PDFDocument24 paginiPiis0002937811009185 PDFLailatuss LelaÎncă nu există evaluări
- Desai STOPMIPDocument13 paginiDesai STOPMIPNedson GundoÎncă nu există evaluări
- OB - 02 - Outcomes of Multifetal ReductionDocument6 paginiOB - 02 - Outcomes of Multifetal Reductionram4a5Încă nu există evaluări
- SYPHILIS in Pregnancy CDCDocument5 paginiSYPHILIS in Pregnancy CDCDiana NeculceaÎncă nu există evaluări
- New England Journal Medicine: The ofDocument10 paginiNew England Journal Medicine: The ofTiffany Rachma PutriÎncă nu există evaluări
- Blindness After Facial Injection: Aesthetic Complications GuidelinesDocument3 paginiBlindness After Facial Injection: Aesthetic Complications Guidelineswoouuw0903Încă nu există evaluări
- Ni Hms 411988Document14 paginiNi Hms 411988woouuw0903Încă nu există evaluări
- Crows On 2009Document29 paginiCrows On 2009woouuw0903Încă nu există evaluări
- Rundown Bamed Clinical MeetingDocument4 paginiRundown Bamed Clinical Meetingwoouuw0903Încă nu există evaluări
- For Information About Installing, Running and Configuring Firefox Including A List of Known Issues and Troubleshooting InformationDocument1 paginăFor Information About Installing, Running and Configuring Firefox Including A List of Known Issues and Troubleshooting Informationwoouuw0903Încă nu există evaluări
- Country Snapshot: Zambia: Essential Package of Health ServicesDocument48 paginiCountry Snapshot: Zambia: Essential Package of Health ServicesMarwa Foud100% (1)
- Antimalarial Activity of Crude Extracts of Artocarpus HeterophyllusDocument3 paginiAntimalarial Activity of Crude Extracts of Artocarpus HeterophyllusFrengkyÎncă nu există evaluări
- Emerging in MalariaDocument8 paginiEmerging in MalariaEmad OsmanÎncă nu există evaluări
- The Antiviral Activities of Artemisinin and Artesunate: ReviewarticleDocument8 paginiThe Antiviral Activities of Artemisinin and Artesunate: ReviewarticlemutearaaÎncă nu există evaluări
- Malaria: DR MD Mamunul Abedin ShimulDocument41 paginiMalaria: DR MD Mamunul Abedin ShimulDr. Mamunul AbedinÎncă nu există evaluări
- Ashley, Phyo - 2018 - Drugs in Development For MalariaDocument19 paginiAshley, Phyo - 2018 - Drugs in Development For MalariaShashank SharanÎncă nu există evaluări
- Role of ACT, S & WHO Guidlines For The Treatment of MalariaDocument34 paginiRole of ACT, S & WHO Guidlines For The Treatment of MalariasalmanÎncă nu există evaluări
- 1 - Uncomplicated Malaria and TreatmentDocument35 pagini1 - Uncomplicated Malaria and Treatmentstivana26Încă nu există evaluări
- Malaria Treatment 2013Document75 paginiMalaria Treatment 2013Rheinny IndrieÎncă nu există evaluări
- Treatment of MalariaDocument49 paginiTreatment of MalariaShanza AmaanÎncă nu există evaluări
- Myanmar Baseline AMTR Outlet Survey Report PDFDocument69 paginiMyanmar Baseline AMTR Outlet Survey Report PDFSukiman Bachtiar Wesso100% (1)
- Anti MalariaDocument49 paginiAnti MalariaYIKI ISAACÎncă nu există evaluări
- MalariaDocument6 paginiMalariaShadab Ahmad KhanÎncă nu există evaluări
- Anti Protozoal P1Document5 paginiAnti Protozoal P1N Gv FcÎncă nu există evaluări
- Artesunate Et AmodiquineDocument11 paginiArtesunate Et Amodiquinemmjs10Încă nu există evaluări
- Jurnal MalariaDocument6 paginiJurnal MalariaHhhÎncă nu există evaluări
- Dr. Paulus Novian Harijanto, SPPD, K-PTI, FINASIM-Management Malaria in SepsisDocument30 paginiDr. Paulus Novian Harijanto, SPPD, K-PTI, FINASIM-Management Malaria in SepsisOlivia DwimaswastiÎncă nu există evaluări
- Arte Sun AteDocument9 paginiArte Sun Atebaitur_rohmah8372Încă nu există evaluări
- Stabilization CentreDocument42 paginiStabilization Centreabdullahi bashiirÎncă nu există evaluări
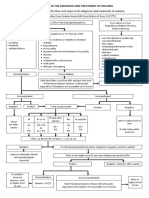
- Algorithm in The Diagnosis and Treatment of MalariaDocument1 paginăAlgorithm in The Diagnosis and Treatment of MalariaPearl Monette Cedeño AngÎncă nu există evaluări
- Gen M Injection-ArtesunateDocument1 paginăGen M Injection-ArtesunateAazar Ali ChannaÎncă nu există evaluări
- Yuan 2021Document34 paginiYuan 2021Sagar PatilÎncă nu există evaluări
- Malaria: Dr. Harun Hudari, SPPDDocument49 paginiMalaria: Dr. Harun Hudari, SPPDEdvans HenryÎncă nu există evaluări
- Nigeria Essential Medicine List For Children 2020Document52 paginiNigeria Essential Medicine List For Children 2020Sadiya Mohammed100% (1)
- Child - Health - in - Developing - Countries 2015-2016 PDFDocument155 paginiChild - Health - in - Developing - Countries 2015-2016 PDFNovi AryandaÎncă nu există evaluări
- Malaria Treatment UpdateDocument45 paginiMalaria Treatment UpdateGyabaah Yeboah AndrewsÎncă nu există evaluări
- MalariaDocument23 paginiMalariaIBhe Damianry QritezzÎncă nu există evaluări