S-ar putea să vă placă și
- Reliability Technoology For Submarine Repeaters PDFDocument8 paginiReliability Technoology For Submarine Repeaters PDFbolermÎncă nu există evaluări
- Trudy Scott Amino-AcidsDocument35 paginiTrudy Scott Amino-AcidsPreeti100% (5)
- CSC Proforma - FeverDocument6 paginiCSC Proforma - Fever127 Shruthik Patel ThotaÎncă nu există evaluări
- 1E Star Trek Customizable Card Game - 6 First Contact Rule SupplementDocument11 pagini1E Star Trek Customizable Card Game - 6 First Contact Rule Supplementmrtibbles100% (1)
- H&P TemplateDocument6 paginiH&P TemplateRicardoMelendezÎncă nu există evaluări
- Health History Documentation Form ChristinaDocument6 paginiHealth History Documentation Form Christinaapi-545542584Încă nu există evaluări
- CDX 1 FinalDocument74 paginiCDX 1 FinalGabby Elardo100% (1)
- History Taking and Physical ExaminationDocument53 paginiHistory Taking and Physical ExaminationBoruuf If GammachuuÎncă nu există evaluări
- Posting ElectiveDocument7 paginiPosting ElectiveThulasi tootsieÎncă nu există evaluări
- Appendix 10 Patient Profile TemplateDocument6 paginiAppendix 10 Patient Profile TemplateAL Rizwan AsifÎncă nu există evaluări
- History and Physical ExaminationDocument17 paginiHistory and Physical ExaminationNur Fatima SanaaniÎncă nu există evaluări
- HAB Manual 2019Document189 paginiHAB Manual 2019anne claire feudo100% (1)
- Varicella Zoster InfectionDocument68 paginiVaricella Zoster InfectionChristelle Brookshiel Demayo Marba100% (1)
- Practical Gastroenterology and Hepatology Board Review ToolkitDe la EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultÎncă nu există evaluări
- 2017 SMDC LeasingDocument2 pagini2017 SMDC Leasingnanobots3767% (3)
- Medicine Case Presentation Pneumonia-CVADocument13 paginiMedicine Case Presentation Pneumonia-CVAJonas Dela CruzÎncă nu există evaluări
- Case Write Up TemplateDocument2 paginiCase Write Up TemplateMohd HadzrieÎncă nu există evaluări
- Family-Oriented Primary CareDocument3 paginiFamily-Oriented Primary Careأحمد خيري التميمي0% (1)
- Nastran 2012 Superelements UgDocument974 paginiNastran 2012 Superelements Ugds_srinivasÎncă nu există evaluări
- Case AnalysisDocument25 paginiCase AnalysisGerly LagutingÎncă nu există evaluări
- GerontologyDocument150 paginiGerontologyKakak wawa95Încă nu există evaluări
- Common Geriatrics - ProblemsDocument91 paginiCommon Geriatrics - ProblemsWafa Abdullah100% (1)
- Theater 10 Syllabus Printed PDFDocument7 paginiTheater 10 Syllabus Printed PDFJim QuentinÎncă nu există evaluări
- Medical Case 1: Language Centre of Malahayati University at 2010Document16 paginiMedical Case 1: Language Centre of Malahayati University at 2010putri1114Încă nu există evaluări
- Hygiene and Ecology TextbookDocument190 paginiHygiene and Ecology Textbookmetzlogan8470Încă nu există evaluări
- Lista Verbelor Regulate - EnglezaDocument5 paginiLista Verbelor Regulate - Englezaflopalan100% (1)
- New Fluid and Electrolytes Therapy Toyinoriginali2againDocument55 paginiNew Fluid and Electrolytes Therapy Toyinoriginali2againt.baby100% (1)
- Summer 2016 MCQDocument16 paginiSummer 2016 MCQDaniel CoyleÎncă nu există evaluări
- Pud Case StudyDocument8 paginiPud Case Studyapi-346620455Încă nu există evaluări
- Fome - Impact of The Illness in A FamilyDocument29 paginiFome - Impact of The Illness in A FamilyMuhammad Gilang DwiputraÎncă nu există evaluări
- Soap Notes HypertensionDocument6 paginiSoap Notes HypertensionCHRISTINE KARENDIÎncă nu există evaluări
- SamplesDocument4 paginiSamplesRalph Lawrence Ruiz Tagorda0% (1)
- BathingDocument34 paginiBathingshannon c. lewisÎncă nu există evaluări
- Becoming A Teacher Someday: Group 4 2G-MTDocument14 paginiBecoming A Teacher Someday: Group 4 2G-MTSophia SaquilayanÎncă nu există evaluări
- Clerking TemplateDocument4 paginiClerking TemplateNur Atiqah Mohd Azli100% (1)
- Pre Authorization FormDocument1 paginăPre Authorization FormMurugan RamalingamÎncă nu există evaluări
- OSCE History Vit B12 Deficiency PDFDocument3 paginiOSCE History Vit B12 Deficiency PDFKashmira JeevaÎncă nu există evaluări
- Practice Guidelines: For Family PhysiciansDocument0 paginiPractice Guidelines: For Family PhysiciansMuhammad GoharÎncă nu există evaluări
- SLMC GC Ipch Osoe (Age) Oct 2019Document4 paginiSLMC GC Ipch Osoe (Age) Oct 2019Alvin FlorentinoÎncă nu există evaluări
- History TakingDocument55 paginiHistory TakingDeepika MahajanÎncă nu există evaluări
- 02 Family Oriented Medical RecordDocument4 pagini02 Family Oriented Medical RecordFernandez-De Ala NicaÎncă nu există evaluări
- Volume 2Document76 paginiVolume 2Muhammad GoharÎncă nu există evaluări
- Case StudiesDocument59 paginiCase Studiesstivana26100% (1)
- Different Injuries of The Musculoskeletal System Its Management and CareDocument113 paginiDifferent Injuries of The Musculoskeletal System Its Management and CareMaAn Castor Palcon TuzonÎncă nu există evaluări
- RNSG 1523 Fluid & Electrolytes Case StudiesDocument2 paginiRNSG 1523 Fluid & Electrolytes Case StudiesDan CamarillasLovesÎncă nu există evaluări
- IM AdconDocument28 paginiIM AdconCla SantosÎncă nu există evaluări
- Case Study #1 ScenarioDocument12 paginiCase Study #1 ScenarioHMG TVÎncă nu există evaluări
- QA PAFP Journal July December 59-2-2021 Pages 115 126Document12 paginiQA PAFP Journal July December 59-2-2021 Pages 115 126Norjetalexis Maningo CabreraÎncă nu există evaluări
- Pedia CaseDocument65 paginiPedia CaseJason MirasolÎncă nu există evaluări
- Cga - 1Document19 paginiCga - 1Kenji Tolero100% (1)
- Department of Pediatrics: Case ProtocolDocument11 paginiDepartment of Pediatrics: Case ProtocolKim Adarem Joy ManimtimÎncă nu există evaluări
- Chronic Hepatitis BDocument9 paginiChronic Hepatitis Bmits98Încă nu există evaluări
- Geriatric AssessmentDocument5 paginiGeriatric AssessmentNurminie Julkipli LÎncă nu există evaluări
- Community Diagnosis: Prepared and Comfiled By: Juanaly Almonte-Badiola, RN, ManDocument87 paginiCommunity Diagnosis: Prepared and Comfiled By: Juanaly Almonte-Badiola, RN, Manjuanamay30gmailcomÎncă nu există evaluări
- Pain at GIDocument74 paginiPain at GIdmtaponÎncă nu există evaluări
- Dermatological History and Examination PDFDocument5 paginiDermatological History and Examination PDFHesbon MomanyiÎncă nu există evaluări
- Clinical Pathology Introductory LectureDocument14 paginiClinical Pathology Introductory Lecture11101955100% (1)
- Chapter 1. History and Physical Examination - Art and ScienceDocument3 paginiChapter 1. History and Physical Examination - Art and SciencecarolineÎncă nu există evaluări
- Ethic ScenariosDocument28 paginiEthic ScenariosQusaiBadrÎncă nu există evaluări
- Pediatrics 2 LaboratoryDocument40 paginiPediatrics 2 LaboratoryAmaetenÎncă nu există evaluări
- Filipino Concept of Health and IllnessDocument43 paginiFilipino Concept of Health and IllnessFelisa Lacsamana Gregorio50% (2)
- 10 Community Oriented Primary CareDocument3 pagini10 Community Oriented Primary CareIrene Veron Bernardo ChicoÎncă nu există evaluări
- Pedia 2017 Case ProtocolDocument14 paginiPedia 2017 Case ProtocolArjay Amba0% (1)
- Nursing Health HistoryDocument2 paginiNursing Health HistoryMahlonee LinÎncă nu există evaluări
- OSCE Stop - Lecture Long HistoryDocument18 paginiOSCE Stop - Lecture Long HistorycrystalsheÎncă nu există evaluări
- Readiness Assurance Test - ANEMIADocument3 paginiReadiness Assurance Test - ANEMIADan Ali0% (1)
- Carbuncle, Incision, Drainage, DebridementDocument11 paginiCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinÎncă nu există evaluări
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutDe la EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutEvaluare: 5 din 5 stele5/5 (1)
- Del Rivera: AUTOMATIC Transmission For Your ConsiderationDocument1 paginăDel Rivera: AUTOMATIC Transmission For Your Considerationnanobots37Încă nu există evaluări
- 11th Annual ConferenceDocument2 pagini11th Annual Conferencenanobots37Încă nu există evaluări
- 2017 SMDC Leasing FaqsDocument3 pagini2017 SMDC Leasing Faqsnanobots37Încă nu există evaluări
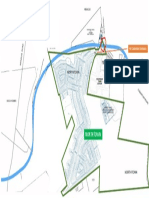
- Northtown: Proposed Bypass Road Affected Entrance SignageDocument1 paginăNorthtown: Proposed Bypass Road Affected Entrance Signagenanobots37Încă nu există evaluări
- Parking and Loading Space RequirementsDocument2 paginiParking and Loading Space Requirementsnanobots37Încă nu există evaluări
- Annex A - Affidavit of Undertaking To Conform - Ver 20180709Document1 paginăAnnex A - Affidavit of Undertaking To Conform - Ver 20180709nanobots37Încă nu există evaluări
- PhilHealth Circular No. 2017-0024 PDFDocument2 paginiPhilHealth Circular No. 2017-0024 PDFnanobots37Încă nu există evaluări
- Locational Clearance FormDocument2 paginiLocational Clearance Formnanobots37Încă nu există evaluări
- Building Permit FormDocument2 paginiBuilding Permit Formnanobots37Încă nu există evaluări
- Barangay Resolution of No ObjectionDocument1 paginăBarangay Resolution of No Objectionnanobots37100% (7)
- Annual Physical ExamDocument1 paginăAnnual Physical Examnanobots37Încă nu există evaluări
- Natural Frequency of Simply Supported STAAD Vs MathCADDocument6 paginiNatural Frequency of Simply Supported STAAD Vs MathCADnanobots37Încă nu există evaluări
- Bridge ConstructionDocument14 paginiBridge Constructionnanobots37Încă nu există evaluări
- PMS Past Paper Pakistan Studies 2019Document3 paginiPMS Past Paper Pakistan Studies 2019AsmaMaryamÎncă nu există evaluări
- CEI and C4C Integration in 1602: Software Design DescriptionDocument44 paginiCEI and C4C Integration in 1602: Software Design Descriptionpkumar2288Încă nu există evaluări
- Joshua 24 15Document1 paginăJoshua 24 15api-313783690Încă nu există evaluări
- Foxit PhantomPDF For HP - Quick GuideDocument32 paginiFoxit PhantomPDF For HP - Quick GuidekhilmiÎncă nu există evaluări
- Diode ExercisesDocument5 paginiDiode ExercisesbruhÎncă nu există evaluări
- A Teacher Must Choose Five Monitors From A Class of 12 Students. How Many Different Ways Can The Teacher Choose The Monitors?Document11 paginiA Teacher Must Choose Five Monitors From A Class of 12 Students. How Many Different Ways Can The Teacher Choose The Monitors?Syed Ali HaiderÎncă nu există evaluări
- Activity Lesson PlanDocument2 paginiActivity Lesson PlanPsiho LoguseÎncă nu există evaluări
- The Hawthorne Studies RevisitedDocument25 paginiThe Hawthorne Studies Revisitedsuhana satijaÎncă nu există evaluări
- Springfield College Lesson Plan Template PHED 237: The Learning and Performance of Physical ActivitiesDocument5 paginiSpringfield College Lesson Plan Template PHED 237: The Learning and Performance of Physical Activitiesapi-285421100Încă nu există evaluări
- Childbirth Self-Efficacy Inventory and Childbirth Attitudes Questionner Thai LanguageDocument11 paginiChildbirth Self-Efficacy Inventory and Childbirth Attitudes Questionner Thai LanguageWenny Indah Purnama Eka SariÎncă nu există evaluări
- The Recipe For Oleander Sou1Document4 paginiThe Recipe For Oleander Sou1Anthony SullivanÎncă nu există evaluări
- Lewin's Change ManagementDocument5 paginiLewin's Change ManagementutsavÎncă nu există evaluări
- Advanced Technical Analysis: - Online Live Interactive SessionDocument4 paginiAdvanced Technical Analysis: - Online Live Interactive SessionmahendarÎncă nu există evaluări
- Information Theory Entropy Relative EntropyDocument60 paginiInformation Theory Entropy Relative EntropyJamesÎncă nu există evaluări
- Lesson 3 The Prodigal SonDocument2 paginiLesson 3 The Prodigal Sonapi-241115908Încă nu există evaluări
- Introduction To ICT EthicsDocument8 paginiIntroduction To ICT EthicsJohn Niño FilipinoÎncă nu există evaluări
- Robot MecanumDocument4 paginiRobot MecanumalienkanibalÎncă nu există evaluări
- Goal Ball Lesson PlanDocument4 paginiGoal Ball Lesson Planapi-378557749100% (1)
- Syllabus/Course Specifics - Fall 2009: TLT 480: Curricular Design and InnovationDocument12 paginiSyllabus/Course Specifics - Fall 2009: TLT 480: Curricular Design and InnovationJonel BarrugaÎncă nu există evaluări
- Is 13779 1999 PDFDocument46 paginiIs 13779 1999 PDFchandranmuthuswamyÎncă nu există evaluări
- Radio Network Parameters: Wcdma Ran W19Document12 paginiRadio Network Parameters: Wcdma Ran W19Chu Quang TuanÎncă nu există evaluări
- Describing LearnersDocument29 paginiDescribing LearnersSongül Kafa67% (3)
- Nature, and The Human Spirit: A Collection of QuotationsDocument2 paginiNature, and The Human Spirit: A Collection of QuotationsAxl AlfonsoÎncă nu există evaluări