IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 13, Issue 9 Ver. VI (Sep. 2014), PP 85-88
www.iosrjournals.org
www.iosrjournals.org 85 | Page
Chlorhexidine - An antiseptic in periodontics
Dr.Poonam Dutt
1
, Dr. Promod Kr Rathore
2
, Dr. Dheeraj Khurana
3
1
(Professor, Dept. of Periodontics, Shree Bankey Bihari Dental college, Ghaziabad, U.P., India)
2
(Senior Lecturer, Dept. of Periodontics, Shree Bankey Bihari Dental college, Ghaziabad, U.P., India)
3
(P.G Student, Dept. of Periodontics, Shree Bankey Bihari Dental college, Ghaziabad, U.P., India)
Abstract: Studies have demonstrated that plaque microorganisms are the primary etiologic factors associated
with human periodontal disease, plaque must be removed on a consistent basis as a preventative measure.
Unfortunately, routine use of oral hygiene aids (e.g. toothbrush, floss, etc.) to control plaque have not been
entirely successful. Accordingly, the search for alternative methods, such as chemotherapeutic agents, to control
plaque has been extensive. Of the many chemical agents that have been evaluated to determine their effects on
plaque, gingivitis and adult periodontitis, Chlorhexidine (CHX) have been successfully introduced and
extensively researched. Chlorhexidine have been used to aid in controlling plaque build- up. They have been
used to complement, not replace mechanical therapy.
Keywords: Antiseptic, Chlorhexidine, Dental Plaque, Periodontitis, Tooth Discolouration.
I. Introduction
As an antimicrobrial agent, chlorhexidine is effective in vitro against both Gram-positive and Gram-
negative bacteria including aerobes and anaerobes and yeasts and fungi.The digluconate of chlorhexidine (1:6-
Di 4'-chlorophenyl-diguani-dohexane) is a synthetic antimicrobial drug which has been widely used as a broad
spectrum antiseptic in clinical and veterinary medicine since 1953(1-3).
They are agents that kill oral microorganisms that cause gingivitis, periodontitis, and caries(4). Its
antibacterial action is due to an increase in cellular membrane permeability followed by coagulation of the
cytoplasmic macromolecules(5). It has also been shown that chlorhexidine can reduce the adherence of
Porphyromonasgingivalis to epithelial cells(6). This effect is probably due to the binding of chlorhexidine to the
bacterial outer membrane and therefore it could have similar results on the adherence of other plaque
bacteria(7).
The most prevalent infectious oral diseases in humans, caries and periodontal diseases, are associated
with dental plaque. The removal of bacterial biofilm is a decisive component in the prevention and treatment of
these diseases. Because of the difficulty to ensure adequate removal of plaque by mechanical means, there is a
great interest in the use of antimicrobial agents to replace or to be adjuncts to the mechanical approaches.
Chlorhexidine (CHX) is one of the most effective antimicrobial agents for plaque control. It is retained in the
oral cavity and is progressively desorbed in bacteriostatic concentrations 8 hours after rinsing. When a low dose
of CHX is used, the cellular trans- port of the bacterial cell is damaged with the creation of pores in the cellular
membrane. In higher concentration, the solution penetrates the bacterial cell and leads to microorganism
destruction(8).
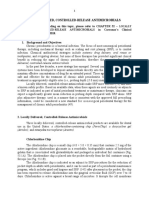
II. Structure
Chlorhexidine (CHX) is a bisbiguanide antiseptic that is a symmetrical molecule consisting of four
chlorophenyl rings and two biguanide groups connected by a central hexamethylene bridge. The compound is a
strong base and is di- cationic at pH levels >3.5, with the two positive charges on either side of the
hexamethylenebridge(9). Several bisguanide antiseptics possess anti-plaque activity, including chlorhexidine,
alexidine andoctenidine. Chlorhexidine gluconate, however, is the most studied bisguanide and is the one on
which there is most information on toxicology. It acts by altering integrity of cell membrane of bacteria. Its
superior anti-plaque activity is the result of its substantivity and pin-cushion effect(10).
III. Substantivity Of Chlorhexidine
The ability of drugs to adsorb onto and bind to soft and hard tissues is known as substantivityand this
property was first described for chlorhexidine in the 1970s.Substantivity is influenced by the concentration of
the medication, its pH and temperature, and the length of time of contact of the solution with the oral structures.
This property of chlorhexidine was associated with its ability to maintain effective concentrations for prolonged
periods of time(11) and this prolongation of its action made it especially suitable for the inhibition of plaque
formation(12).
Chlorhexidine - An antiseptic in periodontics
www.iosrjournals.org 86 | Page
IV. Pin-Cushion Effect
One charged end of Chlorhexidine molecule binding to the tooth surface and the other remaining
available to interact with bacterial membrane as microorganism approaches the tooth surface a pin cushion
effect. This explains the lack of effectiveness of other antimicrobials in terms of them lacking a large, rigid
molecule with two charged interactive ends(13).
V. Metabolism And Toxicity
When Chlorhexidine is used as a mouth rinse the mode of action is purely topical. The drug does not
penetrate oral epithelium and if some solution is inadvertently swallowed, initial binding of the drug will be to
the mucosal surfaces of gastrointestinal tract. Chlorhexidine is poorly absorbed through gastrointestinal tract.
Animal experiments have suggested that Chlorhexidine is mainly excreted through feces. The small amount of
Chlorhexidine that may be absorbed is metabolized in liver and kidney. There is minimal metabolic cleavage.
It is free from systemic toxicity in oral use & microbial resistance & superinfection do not occur. The
oral LD 50 value for Chlorhexidine digluconate is 1800mg/kg, whereas the LD 50 for intravenous application is
22mg/kg(14).
VI. Availability
Over the years, CHX in gels, chips, sprays, and mouth- washes hasbeendeveloped.Ofthese,amouth-
wash is the most commonly used(15).
VII. Use As A Mouthwash
At present, there are 2 commonly used CHX concentration available: one, 0.2% CHX, which is used
with a 10ml volume and the other 0.12% CHX, which is used with a 15ml volume. The rationale for lowering
the concentration of CHX is to reduce side effect while maintaining comparable efficacy. Although the
concentration in these 2 products are different, the total amount of CHX is approximately the same: 10ml of
0.2% CHX contains 20mg and 15ml of 0.12% CHX contain 18mg per volume. Although CHX is an effective
antimicrobial agent in both concentrations(16).
When prescribed, it is recommended that patients rinse twice a day for 30 seconds with 15 mL after
brushing and ossing and after toothpaste has been completely rinsed out of the mouth(4). Chlorhexidine is
recommended as a twice daily, morning and evening, oral rinse to be used for at least 30 seconds. It is not
intended for ingestion and should be expectorated after rinsing(17).
VIII. Use As A Toothpaste
More recently, some toothpastes have been specifically formulated to ensure a high availability of the
contained antiseptic. A 1% chlorhexidine toothpaste of this type has been investigated in a 19- day, randomized
double blind, placebo-controlled, cross-over experimental gingivitis clinical trial. The toothpastes were used as
slurries which were rinsed around the mouth twice per day for 1 minute during the experimental period. Plaque
and gingivitis scores were highly significantly reduced and stain scores were significantly increased in the active
toothpaste period with respect to those in the placebo period. Thus, this particular formulation of chlorhexidine
toothpaste does seem to provide a sufficient dose of chlorhexidine for a similar clinical effect to that seen with
chlorhexidine mouth rinsing(18).
IX. Use As Gum
Chlorhexidine has also been incorporated into a sugar-free chewing gum (Fertin A/S, Vejle, Denmark),
and in this form the chlorhexidine molecule remains unbound. The chewing gum contains 20 mg of
chlorhexidine diacetate and this has been compared with the effects of a 0.2% chlorhexidine mouthwash and a
placebo gum in a clinical study. Therefore, the use of chlorhexidine gum could be a good method of using
chlorhexidine in longer term users(18).
X. Use As Locally Applied Antiseptic
Periochip (Dexcel Pharmaceuticals, Israel) is an orange-brown, biodegradable, rectangular chip
rounded at one end that has an active ingredient of chlorhexidine gluconate (2.5 mg) that is released into the
pocket over a period of 7 to 10 days. It has been found to suppress the pocket ora for up to 11 weeks post
application(4).
Periochip is the only locally applied non-antibiotic antimicrobial approved by the FDA as an adjunct to
SRP procedures for the reduction of probing pocket depth or as part of a routine periodontal maintenance
program. The recommendation for use adjunctive to SRP involves isolation of the periodontal pocket of 5 mm
or more, drying the surrounding area, and grasping the Periochip with a forceps and inserting the chip, curved
Chlorhexidine - An antiseptic in periodontics
www.iosrjournals.org 87 | Page
end rst, into the pocket to its maximum depth. The chip can be maneuvered further into position with a plastic
instrument. One site can be treated per chip(4).
XI. Use As Spray
Sprays could well be used as a replacement for, or an adjunct to, mechanical tooth-brushing. This is
especially true in situations in which mechanical tooth cleaning is impossible and the use of a mouthwash is
difcult or not possible at all. Therefore, indications for the use of CHX spray could include mentally
handicapped patients, elderly persons in nursing homes, patients in intensive care units in hospitals, and patients
with inter-maxillary xation. Sprays have the advantage of focusing delivery at the required site. Therefore,
spray also was advocated for local application in cases of implantology and periodontal surgery(15).
The efcacy of sprays depends on the operator, who should achieve coverage at all sites, as well as the
total dose that is delivered. In this respect, itis interestingtonote that no difference in efcacy was found between
0.2% CHX spray and 0.2% CHX mouthwash. Also, no difference was found between 0.2% spray and 0.12%
mouthwash. No data are available on the comparison of 0.2% and 0.12% sprays in terms of plaque growth
inhibition(15).
XII. Use As Gel
Topical application of Xanthano GEL (CHLO-SITE) which contains a mixture of chlorhexidine
digluconate and dihydrochloride, in a ratio of 1:2.Local administration of chlorhexidine has been demonstrated
to be effective as periodontal therapy. Its mechanism of action includes reduction pellicle formation, alteration
of bacterial adherence to teeth, and alteration of bacterial cell walls which causes cell lysis(19).
XIII. Side Effects
Chlorhexidine is poorly absorbed by the gastrointestinal tract and it therefore dis- plays very low
toxicity (oral LD50 is 1800 mg/kg and the intra- venous LD50 is 22 mg/kg). No tetragenic alterations have been
found following long-term use(18).
The reported side effects of CXH are alteration in taste, increase of calculus formation, staining of teeth
and mucous membranes and, more rarely, oral mucosa desquamation and parotid swelling. However, the most
obvious and important local side effects are the brown staining of the teeth, restorative materials and dorsum of
the tongue as well as supragingival calculus formation.
Non-enzymatic browning (Maillard reactions) and formation of pigmented metal sulfides are
considered the possible mechanisms of tooth discolorations due to CHX application. However, clinical and
laboratory studies provided strong evidence that staining is caused by interaction or precipitation of dietary
chromogens with locally adsorbed CXH. In the presence of food components, CHX dyes produce colored
compounds on hydroxyapatite. Moreover, when associated with tea and coffee intake, brown staining of tooth
and acrylic previously exposed to CXH is more likely to occur. Corroborating these findings, Addyet. al. (1979)
demonstrated that tea, coffee and red wine were particularly chromogenic(20).
The increase of calculus formation due to CHX mouthrinse is a usual finding in early long-term
investigations. However, short-term studies suggested reduced calculus formation with CHX rinsing.The
process of mineralization and the CHX influence on the process are not fully understood, but involves localized
supersaturation, nucleation, crystal growth and the transformation of precursor phases such as dicalcium
phosphate dehydrate, octacalcium phosphate and amorphous calcium phosphate into more stable, crystalline
deposits of hydroxyapatite.However, a recent in vivo study has shown that adjunctive usage of an oxidizing
agent in addition to chlorhexidine reduced such staining and plaque formation and development of
gingivitis(20).
Lesscommonly,CHXcausesmucosalerosion,and this appears idiosyncratic, with the antiseptic effects on
the surface of epithelial cells in some people. Desquamative soft tissue lesions have also been reported with use
of drug concentrations exceeding 0.2% or after prolonged application. Extremely rare but unilateral or bilateral
parotid swelling may occur following use of CHX rinsing, but the mechanism is unknown(17).
For these reasons, the prolonged use of chlorhexidine should be avoided in normal periodontal patients.
It is useful for short periods of up to 2 weeks when oral hygiene may be difficult or impossible, such as during
acute oral infections or following periodontal or other forms of oral surgery. It may occasionally be used as an
adjunct to mechanical oral hygiene in initial periodontal treatment. In this regard, the gingivae may be sore after
subgingival scaling and this may prevent normal tooth brushing. However, this effect does not usually last more
than 2 to 3 days and therefore the use of the mouthwash is not usually necessary for more than this period. At
this point normal brushing and flossing must be resumed and mouthwashing should stop(18).
Chlorhexidine - An antiseptic in periodontics
www.iosrjournals.org 88 | Page
XIV. Conclusion
Chlorhexidine to date is the most potent anti plaque agent. Chlorhexidine and any other potent
antimicrobial agent should be applied only under professional supervision.
References
[1]. G. Davies, J. Francis, A. Martin, F. Rose, G. Swain, 1:6 Di-4-chlorophenldiguanidohexane. Laboratory investigation into a new
antibacterial agent of high potency, Br J Pharmacol, 9, 1954, 192-196.
[2]. T. Hennessy, Some antibacterial properties of chlorhexidine, J Periodont Res, 8(suppl.), 1973, 61-67.
[3]. C. Emisilon, Susceptibility of various microorganisms to chlorhexidine. Scand J Dent Res, 85, 1977, 255-265.
[4]. ME. Ryan, Nonsurgical approaches for the treatment of periodontal diseases, Dent Clin N Am, 49, 2005, 611636.
[5]. T. Hennessy, Antibacterial properties of Hibitane, J ClinPeriodontol, 4, 1977,36-48.
[6]. D. Grenier, Effect of chlorhexidine on the adherence properties of Porphyromonasgingivalis, J ClinPeriodontol, 23, 1996, 140-142.
[7]. P. Hull, Chemical inhibition of plaque, J ClinPeriodontol, 7, 1980, 431-442.
[8]. CAF. Neto, CCF. Parolo, CK. Rsing, M. Maltz, Comparative analysis of the effect of two chlorhexidine mouthrinses on plaque
accumulation and gingival bleeding, Braz Oral Res 22(2), 2008, 139-44.
[9]. L. Flotra,P. Gjermo, G. Rolla, J. Waerhaug, Side effects of chlorhexidine mouthwashes, Scand J Dent Res , 79, 1971, 119-125.
[10]. M. Addy, Chlorhexidine compared with other locally delivered antimicrobials. J ClinPeriodontol, 13,1986, 957964.
[11]. P. Bonesvoll , P. Lkken , G. Rlla, Influence of concentration, time, temperature and pH on the retention of chlorhexidine in the
human oral cavity after mouth rinses. Arch Oral Biol, 19, 1974, 1025-1029.
[12]. Winrow M. Metabolic studies with radiolabelled chlorhexidine in animals and man. J Periodont Res, 12, (suppl.), 1973, 45-48.
[13]. S. Mathur, T. Mathur, R. Srivastava, R. Khatri, Chlorhexidine: The Gold Standard in Chemical Plaque Control, National Journal of
Physiology, Pharmacy & Pharmacology, 1(2), 2011, 45-51.
[14]. E. Faulkers, Some toxicological observations on Chlorhexidine, J. Periodontol Res, 8 (suppl 12), 1973, 55-57.
[15]. JE. Stoeken, PA. Versteeg, NAM. Rosema, MF. Timmerman, U. van der Velden, GA. van der Weijden, Formation With 0.12%
Chlorhexidine Spray Compared to 0.2% Spray and 0.2% Chlorhexidine Mouthwash, J Periodontol, 78, 2007, 899-904.
[16]. JAM. Keijser, H. Verkade, MF. Timmerman, FA. Van der Weijden, Comparison of 2 Commercially Available Chlorhexidine
Mouthrinses, J Periodontol, 74, 2003, 214-218.
[17]. CA. Gurgan, E. Zaim, I. Bakirsoy, E. Soykan, Short-Term Side Effects of 0.2% Alcohol-Free Chlorhexidine Mouthrinse Used as
an Adjunct to Non-Surgical Periodontal Treatment: A Double-Blind Clinical Study, J Periodontol, 77, 2006, 370-384.
[18]. BM. Eley, Antibacterial agents in the control of supragingival plaque a review, British Dent. journal, 186(6), 1999, 286-296.
[19]. MMAJ. Abdaly, ANMEl. Refai, UM. Gouda, HA. Atty, Evaluation of Topical Application of CHLO-SITE (Chlorhexidine gel) in
Management of Chronic Periodontitis, Suez Canal Univ Med J, 11(1), 2008, 35 -40.
[20]. FB. Zanatta, RP. Antoniazzi, CK. Rsing, Staining and calculus formation after 0.12% chlorhexidine rinses in plaque-free and
plaque covered surfaces: a randomized trial, J Appl Oral Sci, 2009, 515-521.
S-ar putea să vă placă și
- Management of Deep Carious LesionsDe la EverandManagement of Deep Carious LesionsFalk SchwendickeÎncă nu există evaluări
- Characteristics, Uses and Side Effects of ChlorhexidineDocument3 paginiCharacteristics, Uses and Side Effects of ChlorhexidinesuhanaÎncă nu există evaluări
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryDe la EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryÎncă nu există evaluări
- Chlorhexidine Mouthwash Review: Antimicrobial Mechanism and Dental ApplicationsDocument3 paginiChlorhexidine Mouthwash Review: Antimicrobial Mechanism and Dental ApplicationsAniend Uchuz ChizÎncă nu există evaluări
- Parenteral Products: The Preparation and Quality Control of Products for InjectionDe la EverandParenteral Products: The Preparation and Quality Control of Products for InjectionÎncă nu există evaluări
- Mouthwashes and Their Use in Different Oral ConditionsDocument6 paginiMouthwashes and Their Use in Different Oral ConditionsReemALMousawiÎncă nu există evaluări
- SJDS 22B186 191 PDFDocument6 paginiSJDS 22B186 191 PDFyudhistira pradiptyaÎncă nu există evaluări
- Kapoor2011Document5 paginiKapoor2011Tiara IkaÎncă nu există evaluări
- Presentation 1Document20 paginiPresentation 1Sambhav JainÎncă nu există evaluări
- Artículo - EnjuaguesDocument12 paginiArtículo - Enjuaguesmariajnavarro2505Încă nu există evaluări
- Mouthwashes and Their Use in Different Oral ConditionsDocument6 paginiMouthwashes and Their Use in Different Oral ConditionsBagus RahmawanÎncă nu există evaluări
- Sajan (2019) Chlorhexidine As An Antimicrobial Agent in Dentistry - A ReviewDocument9 paginiSajan (2019) Chlorhexidine As An Antimicrobial Agent in Dentistry - A ReviewPhuong ThaoÎncă nu există evaluări
- Antibiotic. 2018Document9 paginiAntibiotic. 2018Abas HamzaÎncă nu există evaluări
- Peran Irigasi Klorheksidin Pada Perawatan Penyakit PeriodontalDocument5 paginiPeran Irigasi Klorheksidin Pada Perawatan Penyakit PeriodontalNanda WarizkyÎncă nu există evaluări
- Brookes (2020), Current Uses of Chlorhexidine For Management of Oral Disease: A Narrative ReviewDocument10 paginiBrookes (2020), Current Uses of Chlorhexidine For Management of Oral Disease: A Narrative ReviewPhuong ThaoÎncă nu există evaluări
- 7&8. Chemotherapeutic AgentsDocument74 pagini7&8. Chemotherapeutic AgentsYauÎncă nu există evaluări
- Use of Chlorhexidine Varnishes in Preventing and Treating Periodontal DiseaseDocument4 paginiUse of Chlorhexidine Varnishes in Preventing and Treating Periodontal Diseasetaher adelÎncă nu există evaluări
- CHXMDocument11 paginiCHXMshubhrahulÎncă nu există evaluări
- Anti-Plaque & Anti-Calculus AgentsDocument43 paginiAnti-Plaque & Anti-Calculus AgentsRishabh Madhu SharanÎncă nu există evaluări
- Rinsing With Chlorhexidine Gluconate Solution After Brushing and Ossing Teeth: A Systematic Review of EffectivenessDocument9 paginiRinsing With Chlorhexidine Gluconate Solution After Brushing and Ossing Teeth: A Systematic Review of EffectivenessMariel GentilesÎncă nu există evaluări
- The Role of Cetylpyridinium Chloride Mouthwash in The Treatment of PeriodontitisDocument2 paginiThe Role of Cetylpyridinium Chloride Mouthwash in The Treatment of PeriodontitisinventionjournalsÎncă nu există evaluări
- Paraskevas (2008), Chlorine Dioxide and Chlorhexidine Mouthrinses Compared in A 3-Day Plaque Accumulation ModelDocument6 paginiParaskevas (2008), Chlorine Dioxide and Chlorhexidine Mouthrinses Compared in A 3-Day Plaque Accumulation ModelPhuong ThaoÎncă nu există evaluări
- ChlorhexidineDocument11 paginiChlorhexidineJuan José SantosÎncă nu există evaluări
- Antibacterial Effect of Taurolidine (2%) On Established Dental Plaque BiofilmDocument7 paginiAntibacterial Effect of Taurolidine (2%) On Established Dental Plaque BiofilmDeepshriAgrawalÎncă nu există evaluări
- ChlorhexidineDocument6 paginiChlorhexidineadhamelthnÎncă nu există evaluări
- 2Document50 pagini2rupaliÎncă nu există evaluări
- (53C) Locally Delivered, Controlled-Release AntimicrobialsDocument5 pagini(53C) Locally Delivered, Controlled-Release AntimicrobialsElena Pleșca MunteanuÎncă nu există evaluări
- Chlorhexidine Gluconate, Its Properties and Applications in Endodontics 2008Document15 paginiChlorhexidine Gluconate, Its Properties and Applications in Endodontics 2008Abhishek Isaac MathewÎncă nu există evaluări
- Final Antiseptics PowerpointDocument77 paginiFinal Antiseptics Powerpointalana_sushineÎncă nu există evaluări
- ChlorhexidineDocument21 paginiChlorhexidineKristin CurtisÎncă nu există evaluări
- Efficacy of Natural Antimicrobials in Toothpaste Formulations Against Oral Biofilms in VitroDocument7 paginiEfficacy of Natural Antimicrobials in Toothpaste Formulations Against Oral Biofilms in VitroRobert ShawÎncă nu există evaluări
- Definisi: Chong BS. 2017. Harty's Endodontics in Clinical Practice 7 Ed. Elsevier LTDDocument61 paginiDefinisi: Chong BS. 2017. Harty's Endodontics in Clinical Practice 7 Ed. Elsevier LTDtillahÎncă nu există evaluări
- Chlorhexidine: Still the Gold StandardDocument8 paginiChlorhexidine: Still the Gold StandardPhuong ThaoÎncă nu există evaluări
- Mouthash 10daysDocument7 paginiMouthash 10dayssamanvi badriÎncă nu există evaluări
- Srinu Chemical Plaque ControlDocument80 paginiSrinu Chemical Plaque ControlGorremuchu SrinivasÎncă nu există evaluări
- Formulation and evaluation of medicated chewing gum containing chlorhexidine and chitosanDocument8 paginiFormulation and evaluation of medicated chewing gum containing chlorhexidine and chitosanSher AhmadÎncă nu există evaluări
- Mouthwashes: Camile S Farah, Associate Professor, School of Dentistry and The University ofDocument3 paginiMouthwashes: Camile S Farah, Associate Professor, School of Dentistry and The University ofReemALMousawiÎncă nu există evaluări
- Mouthwashes: Camile S Farah, Associate Professor, School of Dentistry and The University ofDocument3 paginiMouthwashes: Camile S Farah, Associate Professor, School of Dentistry and The University ofHafidzah FaizahÎncă nu există evaluări
- Mustafa UlkerDocument8 paginiMustafa UlkerTasha FarahÎncă nu există evaluări
- The Topical Effect of Chlorhexidine and Povidone-Iodine in The Repair of Oral Wounds. A ReviewDocument7 paginiThe Topical Effect of Chlorhexidine and Povidone-Iodine in The Repair of Oral Wounds. A ReviewMario CastroÎncă nu există evaluări
- Chlorhexidine in Endodontics: Brazilian Dental Journal March 2013Document15 paginiChlorhexidine in Endodontics: Brazilian Dental Journal March 2013Dulgheru StefanÎncă nu există evaluări
- Jop 1986 57 6 370Document8 paginiJop 1986 57 6 370Reynee Shaira MatulacÎncă nu există evaluări
- Advanced Drug Delivery Systems For Local Treatment of The Oral CavityDocument24 paginiAdvanced Drug Delivery Systems For Local Treatment of The Oral CavityanjaÎncă nu există evaluări
- Lafaurie 2018Document8 paginiLafaurie 2018Gregorio Antonio Valero VerdeÎncă nu există evaluări
- 11th JC - SINDHUDocument22 pagini11th JC - SINDHUDadi SindhuÎncă nu există evaluări
- Co 2Document6 paginiCo 2Sitti Nur QomariahÎncă nu există evaluări
- Active Ingredients of MouthwashesDocument8 paginiActive Ingredients of Mouthwashesmostafa adelÎncă nu există evaluări
- DR - Hayder A. Alwaeli: Jordan University of Science & TechnologyDocument49 paginiDR - Hayder A. Alwaeli: Jordan University of Science & Technologyapi-3861216Încă nu există evaluări
- Haydari Et Al 2017Document8 paginiHaydari Et Al 2017Valentina Llanca MejíasÎncă nu există evaluări
- A Review of Chlorhexidine and Its Use in Special PopulationsDocument7 paginiA Review of Chlorhexidine and Its Use in Special PopulationseliasberniÎncă nu există evaluări
- Local Antimicrobial TherapyDocument87 paginiLocal Antimicrobial TherapyDrAbhishek SinhaÎncă nu există evaluări
- Cat WinterDocument2 paginiCat Winterapi-506024957Încă nu există evaluări
- Antibiotic Medicaments ReviewDocument10 paginiAntibiotic Medicaments ReviewGeorge ChackoÎncă nu există evaluări
- Comparative Evaluation of Chlorhexidine and Hydrogen Peroxide Mouth Wash Among Patients With GingivitisDocument5 paginiComparative Evaluation of Chlorhexidine and Hydrogen Peroxide Mouth Wash Among Patients With GingivitisInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Solmaz (2012), Inhibition and Disruption Properties of Chlorhexidine Gluconate On Single and Multispecies Oral BiofilmsDocument6 paginiSolmaz (2012), Inhibition and Disruption Properties of Chlorhexidine Gluconate On Single and Multispecies Oral BiofilmsPhuong ThaoÎncă nu există evaluări
- 360 916 4 PBDocument10 pagini360 916 4 PBPrasanth ManupatiÎncă nu există evaluări
- Dentin in Situ: 0R) KJDQ %, +$1, Sabine KALETA-KRAGT, Preeti SINGH-HÜSGEN, Markus Jörg ALTENBURGER, Stefan ZimmerDocument9 paginiDentin in Situ: 0R) KJDQ %, +$1, Sabine KALETA-KRAGT, Preeti SINGH-HÜSGEN, Markus Jörg ALTENBURGER, Stefan Zimmerrizqi ammaliyyahÎncă nu există evaluări
- 86Document5 pagini86Andrada IonescuÎncă nu există evaluări
- Comparing The Efficacy of Hyper-Pure Chlorine-Dioxide With Other Oral Antiseptics On Oral Pathogen Microorganisms and Biofilm in VitroDocument1 paginăComparing The Efficacy of Hyper-Pure Chlorine-Dioxide With Other Oral Antiseptics On Oral Pathogen Microorganisms and Biofilm in VitroPhuong ThaoÎncă nu există evaluări
- Chlorhexidine & Its UsesDocument40 paginiChlorhexidine & Its UsesSriya Saatwika ReddyÎncă nu există evaluări
- The Effect of Instructional Methods and Locus of Control On Students' Speaking Ability (An Experimental Study in State Senior High School 01, Cibinong Bogor, West Java)Document11 paginiThe Effect of Instructional Methods and Locus of Control On Students' Speaking Ability (An Experimental Study in State Senior High School 01, Cibinong Bogor, West Java)International Organization of Scientific Research (IOSR)Încă nu există evaluări
- Comparison of Psychological Variables Within Different Positions of Players of The State Junior Boys Ball Badminton Players of ManipurDocument4 paginiComparison of Psychological Variables Within Different Positions of Players of The State Junior Boys Ball Badminton Players of ManipurInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Effects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaDocument10 paginiEffects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaInternational Organization of Scientific Research (IOSR)100% (1)
- Study The Changes in Al-Ahwaz Marshal Using Principal Component Analysis and Classification TechniqueDocument9 paginiStudy The Changes in Al-Ahwaz Marshal Using Principal Component Analysis and Classification TechniqueInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Comparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockDocument2 paginiComparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Child Mortality Among Teenage Mothers in OJU MetropolisDocument6 paginiChild Mortality Among Teenage Mothers in OJU MetropolisInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Project Based Learning Tools Development On Salt Hydrolysis Materials Through Scientific ApproachDocument5 paginiProject Based Learning Tools Development On Salt Hydrolysis Materials Through Scientific ApproachInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Philosophical Analysis of The Theories of Punishment in The Context of Nigerian Educational SystemDocument6 paginiPhilosophical Analysis of The Theories of Punishment in The Context of Nigerian Educational SystemInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Necessary Evils of Private Tuition: A Case StudyDocument6 paginiNecessary Evils of Private Tuition: A Case StudyInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Development of Dacum As Identification Technique On Job Competence Based-Curriculum in High Vocational EducationDocument5 paginiDevelopment of Dacum As Identification Technique On Job Competence Based-Curriculum in High Vocational EducationInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Enhancing Pupils' Knowledge of Mathematical Concepts Through Game and PoemDocument7 paginiEnhancing Pupils' Knowledge of Mathematical Concepts Through Game and PoemInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Microencapsulation For Textile FinishingDocument4 paginiMicroencapsulation For Textile FinishingInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Students' Perceptions of Grammar Teaching and Learning in English Language Classrooms in LibyaDocument6 paginiStudents' Perceptions of Grammar Teaching and Learning in English Language Classrooms in LibyaInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Youth Entrepreneurship: Opportunities and Challenges in IndiaDocument5 paginiYouth Entrepreneurship: Opportunities and Challenges in IndiaInternational Organization of Scientific Research (IOSR)100% (1)
- Need of Non - Technical Content in Engineering EducationDocument3 paginiNeed of Non - Technical Content in Engineering EducationInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Geohydrological Study of Weathered Basement Aquifers in Oban Massif and Environs Southeastern Nigeria: Using Remote Sensing and Geographic Information System TechniquesDocument14 paginiGeohydrological Study of Weathered Basement Aquifers in Oban Massif and Environs Southeastern Nigeria: Using Remote Sensing and Geographic Information System TechniquesInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Lipoproteins and Lipid Peroxidation in Thyroid DisordersDocument6 paginiLipoproteins and Lipid Peroxidation in Thyroid DisordersInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Comparison of Selected Anthropometric and Physical Fitness Variables Between Offencive and Defencive Players of Kho-KhoDocument2 paginiComparison of Selected Anthropometric and Physical Fitness Variables Between Offencive and Defencive Players of Kho-KhoInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Auxin Induced Germination and Plantlet Regeneration Via Rhizome Section Culture in Spiranthes Sinensis (Pers.) Ames: A Vulnerable Medicinal Orchid of Kashmir HimalayaDocument4 paginiAuxin Induced Germination and Plantlet Regeneration Via Rhizome Section Culture in Spiranthes Sinensis (Pers.) Ames: A Vulnerable Medicinal Orchid of Kashmir HimalayaInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Comparative Effect of Daily Administration of Allium Sativum and Allium Cepa Extracts On Alloxan Induced Diabetic RatsDocument6 paginiComparative Effect of Daily Administration of Allium Sativum and Allium Cepa Extracts On Alloxan Induced Diabetic RatsInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Advancing Statistical Education Using Technology and Mobile DevicesDocument9 paginiAdvancing Statistical Education Using Technology and Mobile DevicesInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Study of Effect of Rotor Speed, Combing-Roll Speed and Type of Recycled Waste On Rotor Yarn Quality Using Response Surface MethodologyDocument9 paginiStudy of Effect of Rotor Speed, Combing-Roll Speed and Type of Recycled Waste On Rotor Yarn Quality Using Response Surface MethodologyInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Application of Xylanase Produced by Bacillus Megaterium in Saccharification, Juice Clarification and Oil Extraction From Jatropha Seed KernelDocument8 paginiApplication of Xylanase Produced by Bacillus Megaterium in Saccharification, Juice Clarification and Oil Extraction From Jatropha Seed KernelInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Core Components of The Metabolic Syndrome in Nonalcohlic Fatty Liver DiseaseDocument5 paginiCore Components of The Metabolic Syndrome in Nonalcohlic Fatty Liver DiseaseInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Investigation of Wear Loss in Aluminium Silicon Carbide Mica Hybrid Metal Matrix CompositeDocument5 paginiInvestigation of Wear Loss in Aluminium Silicon Carbide Mica Hybrid Metal Matrix CompositeInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Factors Affecting Success of Construction ProjectDocument10 paginiFactors Affecting Success of Construction ProjectInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- A Review On Refrigerants, and Effects On Global Warming For Making Green EnvironmentDocument4 paginiA Review On Refrigerants, and Effects On Global Warming For Making Green EnvironmentInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Research Analysis On Sustainability Opportunities and Challenges of Bio-Fuels Industry in IndiaDocument7 paginiResearch Analysis On Sustainability Opportunities and Challenges of Bio-Fuels Industry in IndiaInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Parametric Optimization of Single Cylinder Diesel Engine For Specific Fuel Consumption Using Palm Seed Oil As A BlendDocument6 paginiParametric Optimization of Single Cylinder Diesel Engine For Specific Fuel Consumption Using Palm Seed Oil As A BlendInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Gingival Index PDFDocument7 paginiGingival Index PDFHamzah SahagÎncă nu există evaluări
- Walsh 2013Document14 paginiWalsh 2013julist.tianÎncă nu există evaluări
- KariesDocument4 paginiKariesSherlocknovÎncă nu există evaluări
- Evaluation of Redox Potential of Herbal Toothpastes: An In-Vitro StudyDocument10 paginiEvaluation of Redox Potential of Herbal Toothpastes: An In-Vitro StudyAthenaeum Scientific PublishersÎncă nu există evaluări
- The Effects of Orthodontic Appliance Base Plate MaterialDocument36 paginiThe Effects of Orthodontic Appliance Base Plate MaterialnaimbariyahÎncă nu există evaluări
- Unit 3 Ap Biology Review GuideDocument23 paginiUnit 3 Ap Biology Review Guideapi-605991044Încă nu există evaluări
- Booklet ListerineDocument8 paginiBooklet Listerineapi-312329159Încă nu există evaluări
- Treatment of Plaque-Induced Gingivitis Chronic PerDocument11 paginiTreatment of Plaque-Induced Gingivitis Chronic PerAlleirbag KajnitisÎncă nu există evaluări
- Mechanism Action of Fluorides II PedoDocument17 paginiMechanism Action of Fluorides II PedoFourthMolar.comÎncă nu există evaluări
- Outline and Learning Outcomes: 22.1 The Gastrointestinal Tract and Its DefensesDocument47 paginiOutline and Learning Outcomes: 22.1 The Gastrointestinal Tract and Its DefenseslilaÎncă nu există evaluări
- Prevention of Dental Caries 1Document38 paginiPrevention of Dental Caries 1Nuran AshrafÎncă nu există evaluări
- Patogenesis dan Patofisiologi Caries dan PulpitisDocument6 paginiPatogenesis dan Patofisiologi Caries dan PulpitisAnonymous 1EQutBÎncă nu există evaluări
- Dental Hygiene Research Paper TopicsDocument4 paginiDental Hygiene Research Paper Topicsgwfdurbnd100% (1)
- Evaluation of The Safety and Efficacy of Over-The-Counter Oral Hygiene Products For The Reduction and Control of Plaque and GingivitisDocument15 paginiEvaluation of The Safety and Efficacy of Over-The-Counter Oral Hygiene Products For The Reduction and Control of Plaque and GingivitisGabriela SolanoÎncă nu există evaluări
- Microbial Complexes in Subgingival Plaque - Socronsky - J Clin Perio 1998Document10 paginiMicrobial Complexes in Subgingival Plaque - Socronsky - J Clin Perio 1998Anjana J PrathapÎncă nu există evaluări
- The Effect of Periodontal Therapy on the Survival Rate and Incidence of Complications of Multirooted Teeth With Furcation Involvement After an Observation Period of at Least 5 Years- A Systematic ReviewDocument14 paginiThe Effect of Periodontal Therapy on the Survival Rate and Incidence of Complications of Multirooted Teeth With Furcation Involvement After an Observation Period of at Least 5 Years- A Systematic ReviewAna Massiel NarváezÎncă nu există evaluări
- The Removable Partial Denture EquationDocument11 paginiThe Removable Partial Denture EquationNony ALkhalifahÎncă nu există evaluări
- 3M - 93C HallTechGuide2191110 PDFDocument21 pagini3M - 93C HallTechGuide2191110 PDFDuvan CastilloÎncă nu există evaluări
- White1997 Dental Calculus Formation EtcDocument16 paginiWhite1997 Dental Calculus Formation EtcJose Salas AdragnaÎncă nu există evaluări
- Adventist University of The PhilippinesDocument12 paginiAdventist University of The PhilippinesJunella MoralesÎncă nu există evaluări
- The Natural Rate of Periodontal Destruction Before Age 40Document14 paginiThe Natural Rate of Periodontal Destruction Before Age 40Gisela De Souza PereiraÎncă nu există evaluări
- BDS Fifth Year & Final Prof. NewDocument4 paginiBDS Fifth Year & Final Prof. NewSumeet SodhiÎncă nu există evaluări
- RPC Dental CareDocument4 paginiRPC Dental Carejvbn2003Încă nu există evaluări
- Dentifrices: An Overview From Past To Present: Dr. Songa Vajra Madhuri and Dr. Lahari BuggapatiDocument4 paginiDentifrices: An Overview From Past To Present: Dr. Songa Vajra Madhuri and Dr. Lahari Buggapatiprabhanshusrivastava2Încă nu există evaluări
- Lecture 6 Diet Nutrients and Dental CariesDocument9 paginiLecture 6 Diet Nutrients and Dental CariesNasser DabiÎncă nu există evaluări
- A Practice-Based Study of A Power ToothbrushDocument7 paginiA Practice-Based Study of A Power ToothbrushbarbiieÎncă nu există evaluări
- Premium C1 Glossary PDFDocument53 paginiPremium C1 Glossary PDFKatarzyna ZawiślakÎncă nu există evaluări
- Nursing Management of Oral HygieneDocument40 paginiNursing Management of Oral HygieneGrace Shabrina HapsariÎncă nu există evaluări
- 2022 English For DentistsDocument108 pagini2022 English For DentistsAlexandru Codrin-IonutÎncă nu există evaluări
- Cet Chews DogsDocument2 paginiCet Chews DogsdougdougdougÎncă nu există evaluări
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesDe la EverandThe Ultimate Guide To Memory Improvement TechniquesEvaluare: 5 din 5 stele5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementDe la EverandTechniques Exercises And Tricks For Memory ImprovementEvaluare: 4.5 din 5 stele4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÎncă nu există evaluări
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 3.5 din 5 stele3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÎncă nu există evaluări
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 5 din 5 stele5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingDe la EverandThe Happiness Trap: How to Stop Struggling and Start LivingEvaluare: 4 din 5 stele4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDe la EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingEvaluare: 5 din 5 stele5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDe la EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingEvaluare: 3.5 din 5 stele3.5/5 (32)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDe la EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsÎncă nu există evaluări
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossDe la EverandThe Tennis Partner: A Doctor's Story of Friendship and LossEvaluare: 4.5 din 5 stele4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDe la EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisEvaluare: 5 din 5 stele5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDe la EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisEvaluare: 5 din 5 stele5/5 (8)