S-ar putea să vă placă și
- Neck Trauma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandNeck Trauma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Hip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Musculoskeletal TraumaDocument12 paginiMusculoskeletal Traumahatem alsrour100% (1)
- PEMBAHASAN EnglishDocument12 paginiPEMBAHASAN EnglishEinz Nur Amalyah IdrusÎncă nu există evaluări
- FracturesDocument4 paginiFracturesJoerich Montesclaros100% (1)
- Orthopaedic EssaysDocument139 paginiOrthopaedic EssaysDuncan Jackson100% (1)
- AMPUTATIONDocument73 paginiAMPUTATIONmohammad farhanÎncă nu există evaluări
- Orthopedic InjuriesDocument27 paginiOrthopedic InjuriesvikramÎncă nu există evaluări
- Percutaneous Osteosynthesis of The Distal Fractures of The Femur. Eladio Saura Mendoza e Eladio Saura SanchezDocument12 paginiPercutaneous Osteosynthesis of The Distal Fractures of The Femur. Eladio Saura Mendoza e Eladio Saura SanchezNuno Craveiro LopesÎncă nu există evaluări
- Diaphyseal Femur FracturesDocument9 paginiDiaphyseal Femur FracturesSoulmates1Încă nu există evaluări
- Maxillofacial TraumaDocument7 paginiMaxillofacial TraumaRegina Desi GresianaÎncă nu există evaluări
- Ortho LMRP 2019Document44 paginiOrtho LMRP 2019skÎncă nu există evaluări
- Clavicle FractureDocument15 paginiClavicle Fracturesalsabil aurellÎncă nu există evaluări
- Frienchzel Joy A. Asis Group 3 BSN 3-ADocument14 paginiFrienchzel Joy A. Asis Group 3 BSN 3-AKenneth Louis GalizaÎncă nu există evaluări
- Litrev SCHDocument7 paginiLitrev SCHdedyalkarni08Încă nu există evaluări
- Anatomy of Spinal CordDocument43 paginiAnatomy of Spinal CordGargi MPÎncă nu există evaluări
- Clavicle Fractures - StatPearls - NCBI BookshelfDocument9 paginiClavicle Fractures - StatPearls - NCBI BookshelfRizqan Fahlevvi AkbarÎncă nu există evaluări
- Selected Instructional Course LecturesDocument27 paginiSelected Instructional Course LecturesAhmad ShakirÎncă nu există evaluări
- Chapter 3Document2 paginiChapter 3ahmadreyhaanÎncă nu există evaluări
- Orthopedic InjuriesDocument24 paginiOrthopedic InjuriesvikramÎncă nu există evaluări
- Spinal Cord InjuryDocument9 paginiSpinal Cord InjurytasneemÎncă nu există evaluări
- Case Report Juli 2013Document21 paginiCase Report Juli 2013NahdiaÎncă nu există evaluări
- Sidhant ThesisDocument109 paginiSidhant ThesisSomeshwar GuptÎncă nu există evaluări
- Actures & DislocationsDocument16 paginiActures & Dislocationssabina_grapiniÎncă nu există evaluări
- College of Nursing Adult Nursing Academic Year Lec. Waleed IbrahimDocument6 paginiCollege of Nursing Adult Nursing Academic Year Lec. Waleed Ibrahimمحمد سعد طه احمدÎncă nu există evaluări
- 1spinal Cord InjuryDocument8 pagini1spinal Cord Injurysunny_jr_Încă nu există evaluări
- Principles of Spine Trauma and Spinal Deformities PDFDocument34 paginiPrinciples of Spine Trauma and Spinal Deformities PDFVirlan Vasile CatalinÎncă nu există evaluări
- Fracture Case AbstractDocument27 paginiFracture Case AbstractMaribel Briones JuanÎncă nu există evaluări
- Proximal Humeral Fracture Repair and RehabilitationDocument8 paginiProximal Humeral Fracture Repair and RehabilitationAnonymous UClts4nYÎncă nu există evaluări
- Fracture and Joint Injuries-General FeaturesDocument19 paginiFracture and Joint Injuries-General Featuresngurah123456789Încă nu există evaluări
- Li LBM 4 Blok 18 AnggunDocument8 paginiLi LBM 4 Blok 18 AnggunAnggun Amanda SaveriiaÎncă nu există evaluări
- Nonunion of FracturesDocument43 paginiNonunion of FracturessharenÎncă nu există evaluări
- Hip FractureDocument4 paginiHip FractureJoel Vertt C. Balboa100% (1)
- Orthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Document13 paginiOrthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Tomas Kurakovas100% (1)
- Fracture ComplicationsDocument11 paginiFracture ComplicationsVALIANT PERMATAPUTRAÎncă nu există evaluări
- Clavicle Fracture - TeachMeSurgeryDocument3 paginiClavicle Fracture - TeachMeSurgeryTeshanKoralageÎncă nu există evaluări
- La Consolacion College Manila: Femoral Neck FractureDocument3 paginiLa Consolacion College Manila: Femoral Neck FractureIvan Liquiran AvenadoÎncă nu există evaluări
- Essay On Fracture ComplicationsDocument9 paginiEssay On Fracture ComplicationsadibahÎncă nu există evaluări
- Femoral Neck FractureDocument19 paginiFemoral Neck FractureTabita P SÎncă nu există evaluări
- 2.supracondylar Humerus FracturesDocument26 pagini2.supracondylar Humerus FracturesDabessa MosissaÎncă nu există evaluări
- Sot 1 2011 6Document4 paginiSot 1 2011 6Erwin CandraÎncă nu există evaluări
- Tibia and Fibula Shaft Fracture in Pediatric Case (Ola)Document20 paginiTibia and Fibula Shaft Fracture in Pediatric Case (Ola)Junarto Putra Tandiarrang100% (1)
- Fracture in Leg Tibia and FibulaDocument27 paginiFracture in Leg Tibia and Fibulachilsya shajiÎncă nu există evaluări
- 116 Muscoskeletal 3NCGroup1Document16 pagini116 Muscoskeletal 3NCGroup1Dud AccÎncă nu există evaluări
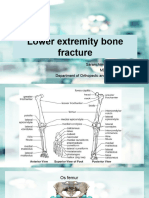
- Lower Extremity Bone Fracture Lecture 3Document88 paginiLower Extremity Bone Fracture Lecture 3Tselmeg TselmegÎncă nu există evaluări
- Ortho Questions 1Document10 paginiOrtho Questions 1Kay BristolÎncă nu există evaluări
- CBD FixDocument17 paginiCBD FixAziir 'arÎncă nu există evaluări
- Pediatric Supracondylar Fractures of The Distal Humerus: Provided by Springer - Publisher ConnectorDocument7 paginiPediatric Supracondylar Fractures of The Distal Humerus: Provided by Springer - Publisher ConnectorBison_sonÎncă nu există evaluări
- 2 - Local Complications of Fractures - D3Document26 pagini2 - Local Complications of Fractures - D3Zainul FatimahÎncă nu există evaluări
- Facial Trauma: Dr. Azher A. Auda Oral and Maxillofacial Surgeon Bds CabsDocument56 paginiFacial Trauma: Dr. Azher A. Auda Oral and Maxillofacial Surgeon Bds CabsHaider F YehyaÎncă nu există evaluări
- 978-0-7817-5096-7 - Chapter 5Document5 pagini978-0-7817-5096-7 - Chapter 5VelventinÎncă nu există evaluări
- Treatment Options of Pelvic and Acetabular Fractures in Patients With Osteoporotic BoneDocument12 paginiTreatment Options of Pelvic and Acetabular Fractures in Patients With Osteoporotic Bonefajri_amienÎncă nu există evaluări
- Mandibular FracturesDocument171 paginiMandibular FracturesBalen ShalawÎncă nu există evaluări
- Clinical Features and Diagnosis of FracturesDocument43 paginiClinical Features and Diagnosis of FracturesChenna Kesava100% (2)
- Hip Fracture: Navigation SearchDocument8 paginiHip Fracture: Navigation SearchjobinbionicÎncă nu există evaluări
- 76040138-Referat-Fraktur-Pelvis EditDocument34 pagini76040138-Referat-Fraktur-Pelvis Editsri wulanÎncă nu există evaluări
- Lowe Limb AmputationDocument11 paginiLowe Limb AmputationNadya ZahraÎncă nu există evaluări
- Anestheticconsiderations Fororal, Maxillofacial, and NecktraumaDocument17 paginiAnestheticconsiderations Fororal, Maxillofacial, and NecktraumaDasubabu GantiÎncă nu există evaluări
- Orthopaedic Essays: Faculty of Medical Sciences Mona CampusDocument185 paginiOrthopaedic Essays: Faculty of Medical Sciences Mona CampusHiruzaminÎncă nu există evaluări
- Treatment of The Fracture of Femur in ChildrenDocument35 paginiTreatment of The Fracture of Femur in Childrenmoaz.zaiter.transporteÎncă nu există evaluări
- 2002 Vol.40 Issues 4 Vascular Imaging PDFDocument278 pagini2002 Vol.40 Issues 4 Vascular Imaging PDFRivani KurniawanÎncă nu există evaluări
- Imaging Acute Abdomen DR - Rivani Kurniawan FixDocument86 paginiImaging Acute Abdomen DR - Rivani Kurniawan FixRivani KurniawanÎncă nu există evaluări
- Intervensi Pulmo Konas Perpari-1Document32 paginiIntervensi Pulmo Konas Perpari-1Rivani KurniawanÎncă nu există evaluări
- Latent TB Infection Provider GuideDocument17 paginiLatent TB Infection Provider GuideRivani KurniawanÎncă nu există evaluări
- Identification and Management of Latent Tuberculosis InfectionDocument8 paginiIdentification and Management of Latent Tuberculosis InfectionRivani KurniawanÎncă nu există evaluări
- Daftar Pustaka 7689Document20 paginiDaftar Pustaka 7689Rivani KurniawanÎncă nu există evaluări
- HI Local Nov07Document15 paginiHI Local Nov07Rivani KurniawanÎncă nu există evaluări
- Bcgletter1 09Document1 paginăBcgletter1 09Rivani KurniawanÎncă nu există evaluări
- Daftar Pustaka bcg098Document6 paginiDaftar Pustaka bcg098Rivani KurniawanÎncă nu există evaluări
- The Epidemiology of Childhood Tuberculosis in The Netherlands: Still Room For PreventionDocument9 paginiThe Epidemiology of Childhood Tuberculosis in The Netherlands: Still Room For PreventionRivani KurniawanÎncă nu există evaluări
- Rhabdomyosarcoma in PediatricDocument2 paginiRhabdomyosarcoma in PediatricRivani KurniawanÎncă nu există evaluări
- TendinitisDocument6 paginiTendinitisRivani KurniawanÎncă nu există evaluări
- Imaging Vesika Seminalis Dan Vas DeferenDocument68 paginiImaging Vesika Seminalis Dan Vas DeferenRivani KurniawanÎncă nu există evaluări
- PP Jurnal Thorak NewDocument93 paginiPP Jurnal Thorak NewRivani KurniawanÎncă nu există evaluări
- Chest Wall TumorDocument27 paginiChest Wall TumorRivani KurniawanÎncă nu există evaluări
- Chest 2003 Jun 123 (6) 2019-27, Figure 3Document1 paginăChest 2003 Jun 123 (6) 2019-27, Figure 3Rivani KurniawanÎncă nu există evaluări
- Skeletal Radiology LengkapDocument89 paginiSkeletal Radiology LengkapRivani KurniawanÎncă nu există evaluări
- GastrointestinalDocument29 paginiGastrointestinalRivani KurniawanÎncă nu există evaluări
- Xiaxi Gb-43: Gall Bladder Channel 1Document2 paginiXiaxi Gb-43: Gall Bladder Channel 1ray72roÎncă nu există evaluări
- U.S. Patent 9,301,519, Entitled, Systems and Methods For Ex Vivo Organ Care, To Hassanein Et Al., Issued Apr. 5, 2016.Document106 paginiU.S. Patent 9,301,519, Entitled, Systems and Methods For Ex Vivo Organ Care, To Hassanein Et Al., Issued Apr. 5, 2016.Anonymous a7S1qyXÎncă nu există evaluări
- HbA1c OdtDocument2 paginiHbA1c OdtAhmed AssafÎncă nu există evaluări
- Deyo 1992Document6 paginiDeyo 1992Wwwanand111Încă nu există evaluări
- Ramatu Kamara ResumeDocument1 paginăRamatu Kamara Resumeapi-707616686Încă nu există evaluări
- General Surgery ConceptsDocument4 paginiGeneral Surgery ConceptsPau De GuzmanÎncă nu există evaluări
- Foundations in Microbiology: TalaroDocument76 paginiFoundations in Microbiology: Talaromertx013Încă nu există evaluări
- Corticosteroids and Associated DiseasesDocument76 paginiCorticosteroids and Associated DiseasesALNAKIÎncă nu există evaluări
- Borax - The Inexpensive Detox, Arthritis, Osteoporosis and Mycoplasma CureDocument14 paginiBorax - The Inexpensive Detox, Arthritis, Osteoporosis and Mycoplasma Curebammer189% (9)
- KDIGO Clinical Practice Guideline On The.9Document93 paginiKDIGO Clinical Practice Guideline On The.9PD18Încă nu există evaluări
- EDiR Notebook (For European Diploma in Radiology)Document250 paginiEDiR Notebook (For European Diploma in Radiology)Parthiban Bala100% (4)
- 26 - Nonsurgical Treatment of Peyronies DiseaseDocument4 pagini26 - Nonsurgical Treatment of Peyronies DiseaseNunuh SulaemanÎncă nu există evaluări
- Sample Nursing Care PlanDocument3 paginiSample Nursing Care Planhyunbin18100% (4)
- Zygomatic Arch and Orbital FracturesDocument6 paginiZygomatic Arch and Orbital FractureszacrouchyÎncă nu există evaluări
- Approach To The Patient With Facial Erythema PDFDocument38 paginiApproach To The Patient With Facial Erythema PDFFilipa FigueiredoÎncă nu există evaluări
- Elc501 - Group Portfolio ForumDocument11 paginiElc501 - Group Portfolio ForumAhmad SyamiÎncă nu există evaluări
- MR - Kuldeep Pandya PDFDocument1 paginăMR - Kuldeep Pandya PDFabhishek mayekarÎncă nu există evaluări
- First Aid For Snake BiteDocument11 paginiFirst Aid For Snake BiteHenryVanDerSchyffÎncă nu există evaluări
- Department of Education: School Contingency PlanDocument14 paginiDepartment of Education: School Contingency PlanClerica RealingoÎncă nu există evaluări
- Fecal Elimination and Urinary EliminationDocument6 paginiFecal Elimination and Urinary Eliminationincent100% (1)
- Group 7 (GIT & Hepatobiliary Case Simulation)Document41 paginiGroup 7 (GIT & Hepatobiliary Case Simulation)Zil Kamleshkumar PanchalÎncă nu există evaluări
- د. هالة Dermatitis-1 (Muhadharaty)Document7 paginiد. هالة Dermatitis-1 (Muhadharaty)adwÎncă nu există evaluări
- 10 Commandments of ConsultationDocument4 pagini10 Commandments of ConsultationZlatan KurjakovicÎncă nu există evaluări
- Dry Fasting The AMAZING Health Benefits Everyone Should Know AboutDocument4 paginiDry Fasting The AMAZING Health Benefits Everyone Should Know AboutMariaÎncă nu există evaluări
- Kshudra Roga Critical Understanding: Dr. Gaurav DesaiDocument39 paginiKshudra Roga Critical Understanding: Dr. Gaurav DesaiDrVikas100% (3)
- Laryngopharyngeal Reflux and Functional Laryngeal Disorder: Perspective and Common Practice of The General GastroenterologistDocument9 paginiLaryngopharyngeal Reflux and Functional Laryngeal Disorder: Perspective and Common Practice of The General GastroenterologistKenzi A HasyaputraÎncă nu există evaluări
- PathogenesisDocument14 paginiPathogenesisIdreesÎncă nu există evaluări
- Modified Ashworth ScaleDocument3 paginiModified Ashworth ScaleSundarajan ManiÎncă nu există evaluări
- v20 n4Document223 paginiv20 n4Sivanantham KrishnamoorthiÎncă nu există evaluări
- K10 - Materi 10 - Tugas CA EBMDocument14 paginiK10 - Materi 10 - Tugas CA EBMputri vivianeÎncă nu există evaluări