S-ar putea să vă placă și
- Psych Drugs Cheat SheetDocument4 paginiPsych Drugs Cheat SheetSunel100% (35)
- UCSF Hospitalist HandbookDocument58 paginiUCSF Hospitalist Handbookniharjhatn100% (1)
- 302 PpJ. Grayson, Freedom From Obsessive Compulsive Disorder A Personalized Recovery Program For LivingDocument2 pagini302 PpJ. Grayson, Freedom From Obsessive Compulsive Disorder A Personalized Recovery Program For LivingMohammad Shoyyad L IkhsanÎncă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Field Attachment Report FinalDocument19 paginiField Attachment Report FinalAmaaca Diva100% (5)
- Gunshot WoundDocument57 paginiGunshot Woundnecrophilia090407Încă nu există evaluări
- 76 Cheat Sheets For Nursing StudentsDocument95 pagini76 Cheat Sheets For Nursing StudentsIly Lagoniya100% (14)
- Hupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine Laura Huppert Full ChapterDocument67 paginiHupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine Laura Huppert Full Chapterannette.reese953100% (6)
- Ebook Hupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine PDF Full Chapter PDFDocument67 paginiEbook Hupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine PDF Full Chapter PDFmartha.delancey633100% (26)
- NursingDocument11 paginiNursingfelixlixan100Încă nu există evaluări
- Dislipid, Hipertensi, Crusade, Grace, Kilip ScoreDocument71 paginiDislipid, Hipertensi, Crusade, Grace, Kilip ScoreWinno Pradana UtomoÎncă nu există evaluări
- Arnons NotesDocument63 paginiArnons Notesmara5140100% (1)
- Lecture Notes On CardiologyDocument31 paginiLecture Notes On CardiologyambiskuysÎncă nu există evaluări
- Robert C. Bourge, M.D., PH.D.: Director Division of Cardiovascular Disease University of AlabamaDocument48 paginiRobert C. Bourge, M.D., PH.D.: Director Division of Cardiovascular Disease University of AlabamaUtomo FemtomÎncă nu există evaluări
- Laporan Kasus Cardio CHF Ec CADDocument14 paginiLaporan Kasus Cardio CHF Ec CADHilyah Fadhilah Al HamdaniÎncă nu există evaluări
- PAC and Hemodynamic Monitoring 2-4-08Document32 paginiPAC and Hemodynamic Monitoring 2-4-08anum786110Încă nu există evaluări
- Aldian Mahendra - CBD DR SaugiDocument109 paginiAldian Mahendra - CBD DR SaugiRobby GumawanÎncă nu există evaluări
- Cardiopulmonary Exercise Testing: Mitchell HorowitzDocument43 paginiCardiopulmonary Exercise Testing: Mitchell Horowitzionanic72Încă nu există evaluări
- Section 09: Interpretation of Clinical GXT Data: ACSM Guidelines: Chapter 6Document34 paginiSection 09: Interpretation of Clinical GXT Data: ACSM Guidelines: Chapter 6Christopher CheathamÎncă nu există evaluări
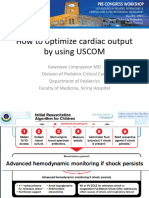
- Uscom by JasonDocument73 paginiUscom by JasonBrotherhood of KryptonianÎncă nu există evaluări
- Regulation of Aterial Blood PressureDocument18 paginiRegulation of Aterial Blood Pressurenihal handÎncă nu există evaluări
- Friday 2-2-2018 CKD HT DMDocument31 paginiFriday 2-2-2018 CKD HT DMJefri SusantoÎncă nu există evaluări
- MNM FebDocument54 paginiMNM FebKevin AgbonesÎncă nu există evaluări
- Anesthesia Monitoring Systems 1Document80 paginiAnesthesia Monitoring Systems 1gnapikaÎncă nu există evaluări
- Critical Care NursingDocument159 paginiCritical Care Nursinggretchen marie80% (5)
- ABSITE CH 16 Critical CareDocument11 paginiABSITE CH 16 Critical CareJames JosephÎncă nu există evaluări
- Medicine OSCE LatestDocument231 paginiMedicine OSCE LatestPrasad HewawasamÎncă nu există evaluări
- Laporan Kasus CHF NYHA III, Diabetes MellitusDocument42 paginiLaporan Kasus CHF NYHA III, Diabetes MellitusGitha Ayu AstarikaÎncă nu există evaluări
- Useful EquationsDocument2 paginiUseful EquationsbidalaÎncă nu există evaluări
- Morning Report: Date: 6 April 2021Document17 paginiMorning Report: Date: 6 April 2021Adinda DianÎncă nu există evaluări
- Post Anesthesia Care Unit (Pacu) : Department of Anesthesiology & Reanimation School of Medicine, Malahayati UniversityDocument46 paginiPost Anesthesia Care Unit (Pacu) : Department of Anesthesiology & Reanimation School of Medicine, Malahayati UniversityIbnu DharmajatiÎncă nu există evaluări
- Thoracicanaesthesia 180527045849Document122 paginiThoracicanaesthesia 180527045849rinduÎncă nu există evaluări
- Duty Report: Sunday, 27 May 2018Document17 paginiDuty Report: Sunday, 27 May 2018HarisÎncă nu există evaluări
- Morning Report: Physician in ChargeDocument29 paginiMorning Report: Physician in ChargeWilujeng AnggrainiÎncă nu există evaluări
- Formulas and Calculations (Study Guide)Document86 paginiFormulas and Calculations (Study Guide)Ravneet singh100% (2)
- Cardiac Output Monitoring - HandoutDocument49 paginiCardiac Output Monitoring - HandoutNakarit SangsirinawinÎncă nu există evaluări
- FormulaeDocument60 paginiFormulaeJoseph FrancisÎncă nu există evaluări
- Hepatopulmonary Syndrome (2014)Document47 paginiHepatopulmonary Syndrome (2014)Robert G. Gish, MDÎncă nu există evaluări
- Lab ValuesDocument6 paginiLab ValuesdnllkzaÎncă nu există evaluări
- Cardiogenic ShockDocument27 paginiCardiogenic ShockMuhammad Ikbar100% (1)
- Sos Pomr SatitiDocument30 paginiSos Pomr SatitiIka AyuÎncă nu există evaluări
- CBD CKD Arif WicaksanaDocument52 paginiCBD CKD Arif WicaksanashabrinaÎncă nu există evaluări
- Follow Up: Tanggal Keluhan/KU/VS Pemeriksaan/Diagnosis Penatalaksanaan 12/3/201 5 06.00 PX Fisik TerapiDocument2 paginiFollow Up: Tanggal Keluhan/KU/VS Pemeriksaan/Diagnosis Penatalaksanaan 12/3/201 5 06.00 PX Fisik TerapiAntonius Bagus BudiÎncă nu există evaluări
- CCRN CardiacDocument39 paginiCCRN CardiacMike100% (5)
- Pulmonary Artery CatheterDocument32 paginiPulmonary Artery Catheterwaqas_xs100% (1)
- Acid Base EquationsDocument21 paginiAcid Base EquationsBen JonesÎncă nu există evaluări
- STEMIDocument28 paginiSTEMIGP HMHÎncă nu există evaluări
- Critical Care NursingDocument159 paginiCritical Care NursingJoy Jarin50% (2)
- Medicine HO Guide Hosp AmpangDocument80 paginiMedicine HO Guide Hosp AmpangMohd Khairie100% (3)
- MR 6 Maret 10Document11 paginiMR 6 Maret 10Arif PrianggaraÎncă nu există evaluări
- ABA OSCE ReviewDocument25 paginiABA OSCE ReviewJohn Smith100% (1)
- Heart Pump and Cardiac Cycle: Faisal I. Mohammed, MD, PHDDocument41 paginiHeart Pump and Cardiac Cycle: Faisal I. Mohammed, MD, PHDUsama SadiqÎncă nu există evaluări
- Surgical Endoscopy Journal 1Document86 paginiSurgical Endoscopy Journal 1Saibo BoldsaikhanÎncă nu există evaluări
- Case Report: Medical Faculty of Hasanuddin University, Makassar 2013Document30 paginiCase Report: Medical Faculty of Hasanuddin University, Makassar 2013ErvinaOctavianiÎncă nu există evaluări
- Arterial Blood Gas: DR - Made Widia, Sp.A (K)Document19 paginiArterial Blood Gas: DR - Made Widia, Sp.A (K)jo_jo_mania100% (1)
- Cardiogenic ShockDocument31 paginiCardiogenic ShockAbdifatah OomaneÎncă nu există evaluări
- Physiology Slides UsmleDocument46 paginiPhysiology Slides Usmlejustseas100% (1)
- Medical Terminology AbbrevDocument16 paginiMedical Terminology AbbrevJaden QuimsonÎncă nu există evaluări
- StemiDocument39 paginiStemiFara OmarÎncă nu există evaluări
- A Clinician - S Guide To Cardiopulmonary Exercise Testing 2 - Test InterpretationDocument23 paginiA Clinician - S Guide To Cardiopulmonary Exercise Testing 2 - Test InterpretationjimurgaÎncă nu există evaluări
- Cardiogenic Shock Part 1Document36 paginiCardiogenic Shock Part 1Martin Miguel AmorÎncă nu există evaluări
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachDe la EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachÎncă nu există evaluări
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationDe la EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationEvaluare: 5 din 5 stele5/5 (2)
- Acute Surgical Topics: An Infographic GuideDe la EverandAcute Surgical Topics: An Infographic GuideÎncă nu există evaluări
- Medical Abbreviations GlossaryDocument15 paginiMedical Abbreviations Glossarydbryant0101100% (9)
- Article Wound DrainsDocument8 paginiArticle Wound DrainsZeynab AbokarÎncă nu există evaluări
- Vancomycin Dosing and Monitoring in AdultsDocument1 paginăVancomycin Dosing and Monitoring in AdultsjulialeoÎncă nu există evaluări
- Parsing Nursing NotesDocument28 paginiParsing Nursing NotesjulialeoÎncă nu există evaluări
- British Heart Journal, 1977, 39, 1019-1025Document7 paginiBritish Heart Journal, 1977, 39, 1019-1025julialeoÎncă nu există evaluări
- Article Wound DrainsDocument8 paginiArticle Wound DrainsZeynab AbokarÎncă nu există evaluări
- Jackson PrattDocument7 paginiJackson PrattjulialeoÎncă nu există evaluări
- Psychiatric Nursing QaDocument20 paginiPsychiatric Nursing QajulialeoÎncă nu există evaluări
- NGT InsertionDocument10 paginiNGT Insertionapi-3722454100% (3)
- Psych NSG Sample QuestionsDocument7 paginiPsych NSG Sample Questionspaul100% (8)
- US Army Medical Course MD0918-100 - Nursing Care Related To The Gastrointestinal and Urinary SystemsDocument137 paginiUS Army Medical Course MD0918-100 - Nursing Care Related To The Gastrointestinal and Urinary SystemsGeorges100% (1)
- Review Notes For NCLEX CGFNS - Aortic AneurysmsDocument2 paginiReview Notes For NCLEX CGFNS - Aortic Aneurysmswyndz100% (3)
- FellowshipbrochureDocument4 paginiFellowshipbrochurejulialeo100% (2)
- Nurse Patient ShipDocument97 paginiNurse Patient Shipcharby12108272100% (2)
- Sickle Cell AnemiaDocument5 paginiSickle Cell Anemiajulialeo100% (2)
- Sickle Cell AnemiaDocument23 paginiSickle Cell AnemiaJesmin_36Încă nu există evaluări
- Review Notes For NCLEX CGFNS - Aortic AneurysmsDocument2 paginiReview Notes For NCLEX CGFNS - Aortic Aneurysmswyndz100% (3)
- Sickle Cell AnemiaDocument10 paginiSickle Cell AnemiaNader Smadi100% (1)
- National Institutes of Health SicklecellbookletDocument16 paginiNational Institutes of Health Sicklecellbookletjulialeo100% (2)
- Sickle Cell AnemiaDocument37 paginiSickle Cell Anemiahazelposis75% (4)
- Triage and Response: Quick LookDocument16 paginiTriage and Response: Quick LookjulialeoÎncă nu există evaluări
- Breast SurgDocument9 paginiBreast SurgjulialeoÎncă nu există evaluări
- PN Dhapter59Document4 paginiPN Dhapter59julialeoÎncă nu există evaluări
- Nursing Test Taking SkillsDocument6 paginiNursing Test Taking SkillsNurseStuffÎncă nu există evaluări
- Triage and Response: Quick LookDocument16 paginiTriage and Response: Quick LookjulialeoÎncă nu există evaluări
- PN Dhapter58Document7 paginiPN Dhapter58julialeoÎncă nu există evaluări
- PN Dhapter57Document5 paginiPN Dhapter57julialeoÎncă nu există evaluări
- Hendry County Complaint, SoFlo AG, LLC.Document16 paginiHendry County Complaint, SoFlo AG, LLC.News-PressÎncă nu există evaluări
- ZENICADocument72 paginiZENICAVedadÎncă nu există evaluări
- Sodium+Bicarbonate Neo v2 0 PDFDocument3 paginiSodium+Bicarbonate Neo v2 0 PDFApres SyahwaÎncă nu există evaluări
- AMORC Index Degrees 5 and 6Document48 paginiAMORC Index Degrees 5 and 6Alois HaasÎncă nu există evaluări
- Otzi ARTEFACTSDocument15 paginiOtzi ARTEFACTSBupe Bareki KulelwaÎncă nu există evaluări
- VSR 421Document2 paginiVSR 421AdarshBijapur0% (1)
- HCM Treatment Italy Ammirati2016Document13 paginiHCM Treatment Italy Ammirati2016xy manÎncă nu există evaluări
- Kisi2 Inggris 11Document3 paginiKisi2 Inggris 11siti RohimahÎncă nu există evaluări
- List of Medical SymptomsDocument6 paginiList of Medical SymptomsAndré Raffael MoellerÎncă nu există evaluări
- Youst TryingDocument5 paginiYoust TryingVictoria Campos GonzálezÎncă nu există evaluări
- Benign Paratesticlar Cyst - A Mysterical FindingDocument2 paginiBenign Paratesticlar Cyst - A Mysterical FindingInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- CDC Org ChartDocument1 paginăCDC Org Chartwelcome martinÎncă nu există evaluări
- Basic Principles of Blending: Selecting Essential OilsDocument3 paginiBasic Principles of Blending: Selecting Essential OilsRullya WindyaÎncă nu există evaluări
- 321 E Lesson 4Document21 pagini321 E Lesson 4Novia eka PutriÎncă nu există evaluări
- Strabismus and Eye Muscle SurgeryDocument68 paginiStrabismus and Eye Muscle SurgeryOpeyemi IdaeworÎncă nu există evaluări
- Patient Education: Colic (Excessive Crying) in Infants (Beyond The Basics)Document15 paginiPatient Education: Colic (Excessive Crying) in Infants (Beyond The Basics)krh5fnjnprÎncă nu există evaluări
- GERD (Gastroesophageal Reflux Disease)Document112 paginiGERD (Gastroesophageal Reflux Disease)Mharj Alfelor Cecilio100% (7)
- Allergic Rhinitis in ChildrenDocument39 paginiAllergic Rhinitis in ChildrenrinajackyÎncă nu există evaluări
- Practice Questions 2Document16 paginiPractice Questions 2Jepe LlorenteÎncă nu există evaluări
- ChitnisDocument1 paginăChitnisAkash Dhiman100% (1)
- Cotton Varieties HybridsDocument15 paginiCotton Varieties HybridsAjay KumarÎncă nu există evaluări
- Review Article Hijamah (Cupping Therapy) - A Comprehensive ReviewDocument8 paginiReview Article Hijamah (Cupping Therapy) - A Comprehensive ReviewMohamed ShiffaÎncă nu există evaluări
- MCQ ChoDocument31 paginiMCQ Choامجد حسين جواد كاظمÎncă nu există evaluări
- Tet PGTRB Zoology Model Question Paper 2Document14 paginiTet PGTRB Zoology Model Question Paper 2Subbarayudu mamillaÎncă nu există evaluări
- Investigation and Treatment of Surgical JaundiceDocument38 paginiInvestigation and Treatment of Surgical JaundiceUjas PatelÎncă nu există evaluări
- How Does Global Warming Affect Our Living?Document19 paginiHow Does Global Warming Affect Our Living?Minahil QaiserÎncă nu există evaluări
- Deenanath Mangeshkar HospitalDocument11 paginiDeenanath Mangeshkar HospitalIti GoyalÎncă nu există evaluări