S-ar putea să vă placă și
- Machine / Plant Checklist Technology Studies: Term 1Document6 paginiMachine / Plant Checklist Technology Studies: Term 1spkumarthÎncă nu există evaluări
- 2 2 e M Checklists PDFDocument15 pagini2 2 e M Checklists PDFKazim NawazÎncă nu există evaluări
- Equipment / Machinery Checklist: BlankDocument3 paginiEquipment / Machinery Checklist: Blankyared admassuÎncă nu există evaluări
- Equipment / Machinery Checklist: BlankDocument4 paginiEquipment / Machinery Checklist: BlankJason Maldonado0% (1)
- Book 1Document6 paginiBook 1Jaime WalkerÎncă nu există evaluări
- Press Machine InspectionDocument5 paginiPress Machine InspectionMichael MiotkÎncă nu există evaluări
- Vehicle Maintenance and Reconditioning LabDocument40 paginiVehicle Maintenance and Reconditioning Labraumil0% (1)
- Air ConditionDocument43 paginiAir ConditionFaquruddin AliÎncă nu există evaluări
- Mac25 Maintenance Section 2Document27 paginiMac25 Maintenance Section 2Wahyu SriharjaÎncă nu există evaluări
- Aeb02012 Ind OEMDocument8 paginiAeb02012 Ind OEM987226146Încă nu există evaluări
- Daily Forklift InspectionDocument1 paginăDaily Forklift InspectionAjai BÎncă nu există evaluări
- Eurocargo Tector 12-26t Repair ManualDocument886 paginiEurocargo Tector 12-26t Repair Manualdieselroarmt875b94% (16)
- Bearing Tester (TSS) - AtcdrivetrainDocument1 paginăBearing Tester (TSS) - AtcdrivetrainSuraj BeheraÎncă nu există evaluări
- Air Handling Unit Construction ChecklistDocument7 paginiAir Handling Unit Construction Checklistameeri143Încă nu există evaluări
- DB Aire Start-Up FormDocument5 paginiDB Aire Start-Up FormAhmed SofaÎncă nu există evaluări
- Nema Frame Motors (17-Samss-503) Pages (1-3) : Saudi Aramco Pre-Commissioning FormDocument13 paginiNema Frame Motors (17-Samss-503) Pages (1-3) : Saudi Aramco Pre-Commissioning FormHaleem Ur Rashid Bangash100% (1)
- Ee03100 Low Voltage SwitchboardDocument25 paginiEe03100 Low Voltage SwitchboardDeepak Verma100% (1)
- Commissioning Form - Crane TruckDocument2 paginiCommissioning Form - Crane TruckKurniawan PriambodoÎncă nu există evaluări
- AHU Start-Up FormDocument4 paginiAHU Start-Up FormAhmed SofaÎncă nu există evaluări
- Shovel ChecklistDocument2 paginiShovel Checklistjamal motaÎncă nu există evaluări
- Non Routine Card-NrcDocument2 paginiNon Routine Card-Nrcpann67% (3)
- Technical Report Checklist - MARINE ENGINESDocument2 paginiTechnical Report Checklist - MARINE ENGINESsary qasimÎncă nu există evaluări
- TM 9 3416 235 14 and PDocument67 paginiTM 9 3416 235 14 and PMikeÎncă nu există evaluări
- Emr Drill PressDocument3 paginiEmr Drill Presswaqas khanÎncă nu există evaluări
- PASS M0 - Maintenance Manual - 2GJA600065 (E)Document8 paginiPASS M0 - Maintenance Manual - 2GJA600065 (E)dwas1314Încă nu există evaluări
- Check List For Movement of TPDocument3 paginiCheck List For Movement of TPManish ChauhanÎncă nu există evaluări
- General Use Fall Protection EquipmentDocument2 paginiGeneral Use Fall Protection EquipmentJuan Carlos NiñoÎncă nu există evaluări
- 01 - 17 - 72 Equipment Form - UnlockedDocument40 pagini01 - 17 - 72 Equipment Form - UnlockedMuthana JalladÎncă nu există evaluări
- ProIV English WordsDocument22 paginiProIV English WordsLa MandulaÎncă nu există evaluări
- ChecklistDocument14 paginiChecklistJoe Andrew100% (1)
- High Efficiency MotorsDocument3 paginiHigh Efficiency MotorsDeclan4Încă nu există evaluări
- Asme Joint Review-Qrr-Uec 2012Document9 paginiAsme Joint Review-Qrr-Uec 2012Keiti Filbrich100% (1)
- Dmax PDFDocument4.266 paginiDmax PDFAdel Abdel-Azim100% (7)
- Oil Analysis Report ExplanationDocument2 paginiOil Analysis Report Explanationzrcjsyll100% (1)
- Wheel Excavator: Model Number Machine SMU Serial Number Inspection Date Dealer Name & CodeDocument5 paginiWheel Excavator: Model Number Machine SMU Serial Number Inspection Date Dealer Name & CodeMario BreguÎncă nu există evaluări
- At22 MaintenanceDocument37 paginiAt22 MaintenancefabuleukalengaÎncă nu există evaluări
- Attachment 4 Fuji CR Imaging EquipmentDocument8 paginiAttachment 4 Fuji CR Imaging EquipmentKimberly Pascual VicmudoÎncă nu există evaluări
- Check List Pulling CableDocument2 paginiCheck List Pulling CableAldeline Sungahid100% (1)
- Requirement of Model AreaDocument5 paginiRequirement of Model AreaNavnath TamhaneÎncă nu există evaluări
- National-CMMS Equipment-Template V09a - 03.30.2012Document244 paginiNational-CMMS Equipment-Template V09a - 03.30.2012Dang NhatÎncă nu există evaluări
- Report of Inspection and Test:: - ) 1yr: - / - 5yrDocument1 paginăReport of Inspection and Test:: - ) 1yr: - / - 5yrHabibulla BavajiÎncă nu există evaluări
- Miles - 24 Months ServiceDocument2 paginiMiles - 24 Months ServicePawluchÎncă nu există evaluări
- 2.6.1.1 AHU - Construction.checklistDocument5 pagini2.6.1.1 AHU - Construction.checklistHiếu Nguyễn100% (1)
- P Pap Forms 4 The DitionDocument8 paginiP Pap Forms 4 The DitionKAMAL BEHLÎncă nu există evaluări
- DPOH Work Shop, Objective, Org. Lay OutDocument33 paginiDPOH Work Shop, Objective, Org. Lay OutJaikanthan DasarathaÎncă nu există evaluări
- Notice of Installation of A Boiler or Pressure VESSEL (An "Object")Document1 paginăNotice of Installation of A Boiler or Pressure VESSEL (An "Object")Mohammed YcfssÎncă nu există evaluări
- DEWA Power Transformer Site Test Report FormatDocument28 paginiDEWA Power Transformer Site Test Report FormatZaheer Ahamed100% (2)
- Aquaseal Factory Qatar: Operations and Maintenance ChecklistDocument1 paginăAquaseal Factory Qatar: Operations and Maintenance ChecklistSafwan MirÎncă nu există evaluări
- Splitting TractorDocument25 paginiSplitting TractorMark Jackaman100% (2)
- Apqp FormsDocument25 paginiApqp FormsgkspÎncă nu există evaluări
- Manufacturer Data ReportDocument3 paginiManufacturer Data Reporthaikal86100% (1)
- Technical Specification Sheet Update Status: 00Document3 paginiTechnical Specification Sheet Update Status: 00KotreshYankanchiÎncă nu există evaluări
- 8d's y 5 Por Que de NissanDocument8 pagini8d's y 5 Por Que de NissanSergio RuizÎncă nu există evaluări
- Halliburton: S S7 JO/5//3Document4 paginiHalliburton: S S7 JO/5//3Khalfan Al HabsiÎncă nu există evaluări
- Sample Weld Audit ChecklistDocument11 paginiSample Weld Audit ChecklistAmb Patrick Oghate100% (2)
- How to Rebuild & Modify Ford C4 & C6 Automatic TransmissionsDe la EverandHow to Rebuild & Modify Ford C4 & C6 Automatic TransmissionsEvaluare: 5 din 5 stele5/5 (5)
- Small Block Chevrolet: Stock and High-Performance RebuildsDe la EverandSmall Block Chevrolet: Stock and High-Performance RebuildsEvaluare: 4 din 5 stele4/5 (6)
- Aviation Maintenance Technician Handbook—Powerplant (2024): FAA-H-8083-32BDe la EverandAviation Maintenance Technician Handbook—Powerplant (2024): FAA-H-8083-32BÎncă nu există evaluări
- GM Automatic Overdrive Transmission Builder's and Swapper's GuideDe la EverandGM Automatic Overdrive Transmission Builder's and Swapper's GuideEvaluare: 4.5 din 5 stele4.5/5 (8)
- Flow Chart For SiFUS Strata Title ApplicationDocument5 paginiFlow Chart For SiFUS Strata Title ApplicationPhang Han XiangÎncă nu există evaluări
- Mercury 150HPDocument5 paginiMercury 150HP이영석0% (1)
- Customer Satisfaction-ICICI Bank-Priyanka DhamijaDocument85 paginiCustomer Satisfaction-ICICI Bank-Priyanka DhamijaVarun GuptaÎncă nu există evaluări
- CH 2 Nature of ConflictDocument45 paginiCH 2 Nature of ConflictAbdullahAlNoman100% (2)
- Agoura Hills DIVISION - 6. - NOISE - REGULATIONSDocument4 paginiAgoura Hills DIVISION - 6. - NOISE - REGULATIONSKyle KimÎncă nu există evaluări
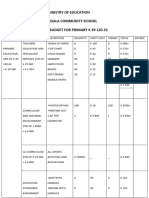
- Ministry of Education Musala SCHDocument5 paginiMinistry of Education Musala SCHlaonimosesÎncă nu există evaluări
- Indictment - 17-Cr-00601-EnV Doc 1 Indictment 11-1-17Document6 paginiIndictment - 17-Cr-00601-EnV Doc 1 Indictment 11-1-17C BealeÎncă nu există evaluări
- Binder 1Document107 paginiBinder 1Ana Maria Gálvez Velasquez0% (1)
- Belimo Fire & Smoke Damper ActuatorsDocument16 paginiBelimo Fire & Smoke Damper ActuatorsSrikanth TagoreÎncă nu există evaluări
- Purchases + Carriage Inwards + Other Expenses Incurred On Purchase of Materials - Closing Inventory of MaterialsDocument4 paginiPurchases + Carriage Inwards + Other Expenses Incurred On Purchase of Materials - Closing Inventory of MaterialsSiva SankariÎncă nu există evaluări
- White Button Mushroom Cultivation ManualDocument8 paginiWhite Button Mushroom Cultivation ManualKhurram Ismail100% (4)
- Ticket Udupi To MumbaiDocument2 paginiTicket Udupi To MumbaikittushuklaÎncă nu există evaluări
- 88 - 02 Exhaust Manifold Gasket Service BulletinDocument3 pagini88 - 02 Exhaust Manifold Gasket Service BulletinGerrit DekkerÎncă nu există evaluări
- Bank of AmericaDocument1 paginăBank of AmericaBethany MangahasÎncă nu există evaluări
- Communication On The Telephone InfoDocument30 paginiCommunication On The Telephone Infomelese100% (1)
- OrganometallicsDocument53 paginiOrganometallicsSaman KadambÎncă nu există evaluări
- Exoskeleton ArmDocument5 paginiExoskeleton Armc214ocÎncă nu există evaluări
- Dr. Najeebuddin Ahmed: 969 Canterbury Road, Lakemba, Sydney, NSW, Australia, 2195Document2 paginiDr. Najeebuddin Ahmed: 969 Canterbury Road, Lakemba, Sydney, NSW, Australia, 2195Najeebuddin AhmedÎncă nu există evaluări
- SPC Abc Security Agrmnt PDFDocument6 paginiSPC Abc Security Agrmnt PDFChristian Comunity100% (3)
- Portfolio Report Zarin Tasnim Tazin 1920143 8Document6 paginiPortfolio Report Zarin Tasnim Tazin 1920143 8Fahad AlfiÎncă nu există evaluări
- ML7999A Universal Parallel-Positioning Actuator: FeaturesDocument8 paginiML7999A Universal Parallel-Positioning Actuator: Featuresfrank torresÎncă nu există evaluări
- Bug Head - Fromjapanese To EnglishDocument20 paginiBug Head - Fromjapanese To EnglishAnonymous lkkKgdÎncă nu există evaluări
- Ver Notewin 10Document5 paginiVer Notewin 10Aditya SinghÎncă nu există evaluări
- Project Job Number EngineerDocument2 paginiProject Job Number Engineertekno plus banatÎncă nu există evaluări
- Preventing OOS DeficienciesDocument65 paginiPreventing OOS Deficienciesnsk79in@gmail.comÎncă nu există evaluări
- Floor Paln ModelDocument15 paginiFloor Paln ModelSaurav RanjanÎncă nu există evaluări
- La Salle Lipa Integrated School Senior High School Community 1 Quarter Summative Assessment Earth Science AY 2021-2022 Household Conservation PlanDocument4 paginiLa Salle Lipa Integrated School Senior High School Community 1 Quarter Summative Assessment Earth Science AY 2021-2022 Household Conservation PlanKarlle ObviarÎncă nu există evaluări
- Interest Rates and Bond Valuation: All Rights ReservedDocument22 paginiInterest Rates and Bond Valuation: All Rights ReservedAnonymous f7wV1lQKRÎncă nu există evaluări
- C Sharp Logical TestDocument6 paginiC Sharp Logical TestBogor0251Încă nu există evaluări
- PartitionDocument5 paginiPartitionKotagiri AravindÎncă nu există evaluări