S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Navigator - Issue 23 PDFDocument19 paginiThe Navigator - Issue 23 PDFuserscribd2011Încă nu există evaluări
- Xxii Paper 05Document8 paginiXxii Paper 05userscribd2011Încă nu există evaluări
- Challenging The She' Culture in The Russian Federation: Symposium Series No. 54 © 2008 IchemeDocument11 paginiChallenging The She' Culture in The Russian Federation: Symposium Series No. 54 © 2008 Ichemeuserscribd2011Încă nu există evaluări
- Buncefield Legal ImpactsDocument13 paginiBuncefield Legal Impactschetan_7927Încă nu există evaluări
- WilkinsonDocument38 paginiWilkinsonuserscribd2011Încă nu există evaluări
- Xxiii Paper 43Document12 paginiXxiii Paper 43userscribd2011Încă nu există evaluări
- 1400 - Isimite - Dynamic Simulation of Texas City Refinery Explosion For Safety StudiesDocument17 pagini1400 - Isimite - Dynamic Simulation of Texas City Refinery Explosion For Safety Studiesuserscribd2011Încă nu există evaluări
- Ods2010 KK BrodieDocument17 paginiOds2010 KK Brodieuserscribd2011Încă nu există evaluări
- Deepwater Horizon - Lessons Learned For The Norwegian Petroleum Industry With Focus On Technical AspectsDocument6 paginiDeepwater Horizon - Lessons Learned For The Norwegian Petroleum Industry With Focus On Technical Aspectsamal118Încă nu există evaluări
- 1383Document80 pagini1383userscribd2011Încă nu există evaluări
- The 1D Iterative Model For Predicting Thermal Radiation From A Jet FireDocument11 paginiThe 1D Iterative Model For Predicting Thermal Radiation From A Jet Fireuserscribd2011Încă nu există evaluări
- ErgoDocument1 paginăErgouserscribd2011Încă nu există evaluări
- 1230 - Ewan - Study of Pressure Safety Valve Response Times Under Transient OverpressuresDocument26 pagini1230 - Ewan - Study of Pressure Safety Valve Response Times Under Transient Overpressuresuserscribd2011Încă nu există evaluări
- 1299Document51 pagini1299userscribd2011100% (2)
- BP OMAR Case Study WebDocument2 paginiBP OMAR Case Study Webuserscribd2011Încă nu există evaluări
- Ageing InstallationsDocument28 paginiAgeing Installationsuserscribd2011Încă nu există evaluări
- 1100 - Oshiro - Decision Making Using Human Reliability AnalysisDocument34 pagini1100 - Oshiro - Decision Making Using Human Reliability Analysisuserscribd2011Încă nu există evaluări
- 1600 - Brocklebank - CDOIF Environmental Risk Tolerability For COMAH EstablishmentsDocument17 pagini1600 - Brocklebank - CDOIF Environmental Risk Tolerability For COMAH Establishmentsuserscribd2011Încă nu există evaluări
- 1500 - Evans - Corporate Memory Collective IntelligenceDocument17 pagini1500 - Evans - Corporate Memory Collective Intelligenceuserscribd2011Încă nu există evaluări
- NeDocument5 paginiNeuserscribd2011Încă nu există evaluări
- 1200 - Brazier - Linking Task Analysis With Other Process Safety ActivitiesDocument15 pagini1200 - Brazier - Linking Task Analysis With Other Process Safety Activitiesuserscribd2011Încă nu există evaluări
- 1130 - Allford - Process Safety AuditingDocument15 pagini1130 - Allford - Process Safety Auditinguserscribd2011Încă nu există evaluări
- BMTWBM OilGas CFD Consequence 2013 WebsiteDocument2 paginiBMTWBM OilGas CFD Consequence 2013 Websiteuserscribd2011Încă nu există evaluări
- Risk Criteria - When Is Low Enough Good Enough - SaudiDocument8 paginiRisk Criteria - When Is Low Enough Good Enough - Saudiuserscribd2011Încă nu există evaluări
- 1100 - Amyotte - No Such Thing As A Black Swan Process IncidentDocument24 pagini1100 - Amyotte - No Such Thing As A Black Swan Process Incidentuserscribd2011Încă nu există evaluări
- 1100 - Forbes - Safety Case On A PageDocument11 pagini1100 - Forbes - Safety Case On A Pageuserscribd2011Încă nu există evaluări
- Review of The Robustness of Epoxy Passive Fire Protection Tech PaperDocument19 paginiReview of The Robustness of Epoxy Passive Fire Protection Tech Paperuserscribd2011100% (1)
- ASFP Talk June 2005 - Copy For ASFPDocument18 paginiASFP Talk June 2005 - Copy For ASFPuserscribd2011Încă nu există evaluări
- DNV Position Paper On Key Aspects of An Effective U S Offshore Safety Regime 22 July 2010Document14 paginiDNV Position Paper On Key Aspects of An Effective U S Offshore Safety Regime 22 July 2010userscribd2011Încă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- MP Aquaversa Below Sink Av ManualDocument26 paginiMP Aquaversa Below Sink Av ManualCarliko FafernerÎncă nu există evaluări
- Combi WRDocument93 paginiCombi WREdinson FlorianoÎncă nu există evaluări
- Maintenance of Handbook Centrifugal PumpDocument34 paginiMaintenance of Handbook Centrifugal Pumpabu naufalÎncă nu există evaluări
- APT14, APT14HC and APT14SHC Automatic Pump Traps: Design Compliance StandardsDocument9 paginiAPT14, APT14HC and APT14SHC Automatic Pump Traps: Design Compliance StandardsmodulofrikiÎncă nu există evaluări
- Flow Over Wiers: Water Chanel Vernier HookDocument4 paginiFlow Over Wiers: Water Chanel Vernier HookEsra BelhajÎncă nu există evaluări
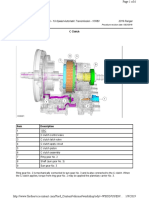
- 307-01 Automatic Transmission 10 Speed - Description and Operation - C ClutchDocument6 pagini307-01 Automatic Transmission 10 Speed - Description and Operation - C ClutchCARLOS LIMADA100% (1)
- Diesel Inspection Testing FormDocument6 paginiDiesel Inspection Testing Form5463RÎncă nu există evaluări
- Pinnacle PCXDocument9 paginiPinnacle PCXMerck Millipore Brasil - Lab Supply BrasilÎncă nu există evaluări
- Shunt ReactorsDocument27 paginiShunt Reactorsarshad262100% (1)
- Bambi Bucket Operations ManualDocument26 paginiBambi Bucket Operations ManualJessica Brown100% (1)
- CHA 550, 660, 1100 WITHOUT CABIN Operation: B 05310 - 1 GB 0897 / MAH 1Document11 paginiCHA 550, 660, 1100 WITHOUT CABIN Operation: B 05310 - 1 GB 0897 / MAH 1João GuardadoÎncă nu există evaluări
- 098 YVAValveDocument2 pagini098 YVAValvesalekojic5332Încă nu există evaluări
- BA Sauer 90R100 H1 enDocument60 paginiBA Sauer 90R100 H1 enTecnico Carretillas Bi BatÎncă nu există evaluări
- Iron Provapor ®Document6 paginiIron Provapor ®pukymottoÎncă nu există evaluări
- Pipeline Design Consideration and StandardsDocument14 paginiPipeline Design Consideration and StandardsSakthivel Swaminathan0% (1)
- Im-1-B Instruction Manual (Vol. I) For Main Engine PDFDocument714 paginiIm-1-B Instruction Manual (Vol. I) For Main Engine PDFДанил КокошенкоÎncă nu există evaluări
- Air Admittance Valves (Ventapipe) : SectionDocument5 paginiAir Admittance Valves (Ventapipe) : SectionDinesh GuptaÎncă nu există evaluări
- Bentley - Modelling Francis Turbine PDFDocument17 paginiBentley - Modelling Francis Turbine PDFAsif MuhammadÎncă nu există evaluări
- Anaesthesia MachineDocument7 paginiAnaesthesia Machinecardiacanesthesia100% (1)
- Antisurge Control SystemDocument10 paginiAntisurge Control Systemsopan saÎncă nu există evaluări
- Petersenplgpckrcats PDFDocument112 paginiPetersenplgpckrcats PDFEdixon ZambranoÎncă nu există evaluări
- Spray-Type Deaerating Heaters: TABLE 12.2Document2 paginiSpray-Type Deaerating Heaters: TABLE 12.2Yanuar KrisnahadiÎncă nu există evaluări
- R22 Info PDFDocument92 paginiR22 Info PDFcoyote556Încă nu există evaluări
- Consult-Spec BIM Integrated DesignDocument62 paginiConsult-Spec BIM Integrated DesignMohammed O. Al-DushyÎncă nu există evaluări
- Radial Pump JD PDFDocument155 paginiRadial Pump JD PDFLeo Vega100% (1)
- DesuperheatersDocument8 paginiDesuperheatersmuhdrijasmÎncă nu există evaluări
- Doosan Compressor HP375WJD, XP375WJD and P425WJDDocument126 paginiDoosan Compressor HP375WJD, XP375WJD and P425WJDJonh Dayrus Ventura AlvarezÎncă nu există evaluări
- Citizen's Charter: Bharat Petroleum Corporation Limited अक्टूबि 2014 October 2014Document57 paginiCitizen's Charter: Bharat Petroleum Corporation Limited अक्टूबि 2014 October 2014Murtaza ShaikhÎncă nu există evaluări
- DR580 PM 733609 07142014 PDFDocument382 paginiDR580 PM 733609 07142014 PDFGabo Gabo100% (3)
- Double Block and Bleed With Ultra-Low Emission Options: Catalog 4190-FPDocument17 paginiDouble Block and Bleed With Ultra-Low Emission Options: Catalog 4190-FPAnandÎncă nu există evaluări