S-ar putea să vă placă și
- Systemic Rituals in Sexual Therapy by Gary L. SandersDocument17 paginiSystemic Rituals in Sexual Therapy by Gary L. SandersOlena BaevaÎncă nu există evaluări
- Counselling Partners and Relatives of Individuals who have Sexually Offended: A Strengths-Focused Eclectic ApproachDe la EverandCounselling Partners and Relatives of Individuals who have Sexually Offended: A Strengths-Focused Eclectic ApproachÎncă nu există evaluări
- The Spotlight Effect in Social Judgment. An Egocentric Bias in Estimates of The Salience of One's Own Actions and AppearanceDocument12 paginiThe Spotlight Effect in Social Judgment. An Egocentric Bias in Estimates of The Salience of One's Own Actions and AppearanceanotherleecherÎncă nu există evaluări
- The Emotionally Abused and Neglected Child: Identification, Assessment and Intervention: A Practice HandbookDe la EverandThe Emotionally Abused and Neglected Child: Identification, Assessment and Intervention: A Practice HandbookÎncă nu există evaluări
- Corporal Punishment by ParentsDocument41 paginiCorporal Punishment by ParentsTim Taliaferro67% (3)
- How I Got This Way and What to Do About ItDe la EverandHow I Got This Way and What to Do About ItÎncă nu există evaluări
- Corporal PunishmentDocument4 paginiCorporal PunishmentDaria GołdaÎncă nu există evaluări
- Applied Human Behavioural Power and Sexual Dynamics: The Book of Social and Sexual Dominance -De la EverandApplied Human Behavioural Power and Sexual Dynamics: The Book of Social and Sexual Dominance -Încă nu există evaluări
- Simon Z. Weismantel From Sadomasochism To BDSM - Rethinking PDFDocument95 paginiSimon Z. Weismantel From Sadomasochism To BDSM - Rethinking PDFJohn C. YoungÎncă nu există evaluări
- Intimacy Undone: Marriage, Divorce and Family Law In IndiaDe la EverandIntimacy Undone: Marriage, Divorce and Family Law In IndiaÎncă nu există evaluări
- Focusing on Physical Sensations During ProcessingDocument2 paginiFocusing on Physical Sensations During Processingaaandrade100% (1)
- Gender StudiesDocument21 paginiGender StudiesAnonymous ocRr3W5NÎncă nu există evaluări
- Arousal and AssaultDocument7 paginiArousal and Assaultmysterix01100% (1)
- Shame. Jim BowlerDocument9 paginiShame. Jim BowlerFrancisco Javier Jiménez BuendíaÎncă nu există evaluări
- Sib AbuseDocument19 paginiSib AbuseUren Don BalamiÎncă nu există evaluări
- Psychology & Sexuality: Click For UpdatesDocument19 paginiPsychology & Sexuality: Click For UpdatesAgustín LiarteÎncă nu există evaluări
- Masochism As A Spiritual JourneyDocument3 paginiMasochism As A Spiritual JourneyDorothy HaydenÎncă nu există evaluări
- Physical AbuseDocument22 paginiPhysical Abuseapi-488921713Încă nu există evaluări
- The Social Construction of BDSMDocument12 paginiThe Social Construction of BDSMleonardo_arceÎncă nu există evaluări
- Havighurtst TheoryDocument4 paginiHavighurtst TheoryGarima KaushikÎncă nu există evaluări
- Boys and Men Healing Documentary/the Healing Years Documentary ReviewsDocument2 paginiBoys and Men Healing Documentary/the Healing Years Documentary ReviewsbigvoicepicturesÎncă nu există evaluări
- Impact of Child Abuse Parenting FemaleDocument5 paginiImpact of Child Abuse Parenting FemaleAffan PresentationsÎncă nu există evaluări
- Transference and Countertransference 2Document24 paginiTransference and Countertransference 2Vipul NagnesiaÎncă nu există evaluări
- Effective Treatment of ExhibitionismDocument2 paginiEffective Treatment of Exhibitionismex1617Încă nu există evaluări
- Defense MechanismsDocument6 paginiDefense MechanismsChris John Cabaluna CogalitoÎncă nu există evaluări
- Complete Well-Being Survey in 10 MinutesDocument7 paginiComplete Well-Being Survey in 10 MinuteslawoffistsÎncă nu există evaluări
- Ocd vs. OcpdDocument1 paginăOcd vs. OcpdIanjoyce OlivarÎncă nu există evaluări
- DealingWith Masochistic Thoughts and BehaviorsDocument18 paginiDealingWith Masochistic Thoughts and BehaviorsΘελξινόη Θελξινοη100% (1)
- Psychological Theories of Sexuality and Human BehaviourDocument26 paginiPsychological Theories of Sexuality and Human Behaviourbinu pereraÎncă nu există evaluări
- Healing Your Shame and Guilt Through Self-ForgivenessDocument7 paginiHealing Your Shame and Guilt Through Self-ForgivenessBook Reader100% (1)
- Family of Origin, Attachment, and Genogram AFT PDFDocument24 paginiFamily of Origin, Attachment, and Genogram AFT PDFtmilic6Încă nu există evaluări
- 1995 Rosenberg Et Al - Global and Specific Self EsteemDocument17 pagini1995 Rosenberg Et Al - Global and Specific Self EsteemnebunikandreeaÎncă nu există evaluări
- Personality TheoriesDocument296 paginiPersonality Theoriessvts100% (1)
- Traumagenic DynamicsDocument20 paginiTraumagenic DynamicsChristian ErrylÎncă nu există evaluări
- Baker Et Al - Kinky Clients, Kinky CounsellingDocument37 paginiBaker Et Al - Kinky Clients, Kinky CounsellingJordan McArthurÎncă nu există evaluări
- 28 SelfRegulation Meditation@0Document4 pagini28 SelfRegulation Meditation@0zhigpÎncă nu există evaluări
- Phases of The Sexual ResponseDocument3 paginiPhases of The Sexual ResponseFaizah Betty RahayuningsihÎncă nu există evaluări
- Human Sexual Behaviour - Britannica Online EncyclopediaDocument25 paginiHuman Sexual Behaviour - Britannica Online EncyclopediaMiruScribd100% (1)
- TEORI MULTIMODALDocument51 paginiTEORI MULTIMODALRidzwan AfiffuddinÎncă nu există evaluări
- A History Of Sex - Simone De Beauvoir's Views On Biology, Psychoanalysis & FeminismDocument15 paginiA History Of Sex - Simone De Beauvoir's Views On Biology, Psychoanalysis & FeminismDaniel Felipe Gutiérrez ÁlvarezÎncă nu există evaluări
- Bystander InterventionDocument5 paginiBystander InterventionMr Mat100% (2)
- Treating Child Sexual AbuseDocument24 paginiTreating Child Sexual AbuseCristina TulbaÎncă nu există evaluări
- Child Sexual Abuse in India Current IssuesDocument3 paginiChild Sexual Abuse in India Current IssuesEditor IJTSRDÎncă nu există evaluări
- BDSM and Helpseeking: Uckland Niversity of EchnologyDocument52 paginiBDSM and Helpseeking: Uckland Niversity of Echnologyadventure of Jay KhatriÎncă nu există evaluări
- The Benefits of Physical PunishmentDocument2 paginiThe Benefits of Physical PunishmentAmb SesayÎncă nu există evaluări
- Repetition Compulsion PDFDocument5 paginiRepetition Compulsion PDFJJÎncă nu există evaluări
- Olweus Sample Standard School ReportDocument72 paginiOlweus Sample Standard School ReportEster RavinskaÎncă nu există evaluări
- America MasochismDocument23 paginiAmerica MasochismJESUS AYLLONÎncă nu există evaluări
- Kinaesthetic Change PDFDocument22 paginiKinaesthetic Change PDFGabriella SalzÎncă nu există evaluări
- Youth: Its Education, Regimen, and Hygiene by Hall, G. Stanley, 1846-1924Document226 paginiYouth: Its Education, Regimen, and Hygiene by Hall, G. Stanley, 1846-1924Gutenberg.orgÎncă nu există evaluări
- Defense Mechanisms: Macalinao, Jay Vee P. BS Psychology 3-1 PSYC 3183 Clinical PsychologyDocument16 paginiDefense Mechanisms: Macalinao, Jay Vee P. BS Psychology 3-1 PSYC 3183 Clinical PsychologyJames JacolbiaÎncă nu există evaluări
- Carl RogersDocument2 paginiCarl RogersAndrew BuckÎncă nu există evaluări
- Case Study of Social PhobiaDocument1 paginăCase Study of Social PhobiaSarah KhairinaÎncă nu există evaluări
- Charlotta Carlström (2019) BDSM Becoming and The Flows of DesireDocument13 paginiCharlotta Carlström (2019) BDSM Becoming and The Flows of DesireAgustín LiarteÎncă nu există evaluări
- A Life Without Stigma: A SANE ReportDocument36 paginiA Life Without Stigma: A SANE ReportSANE Australia100% (5)
- Interpersonal TheoryDocument8 paginiInterpersonal TheoryKenneth ObrienÎncă nu există evaluări
- Shame AttacksDocument11 paginiShame AttacksNata ValleÎncă nu există evaluări
- Communication Skills Journal Assessment TemplateDocument10 paginiCommunication Skills Journal Assessment Templateapi-573661270100% (1)
- Sadism Articlecjp Oct 08 Federoff IRDocument11 paginiSadism Articlecjp Oct 08 Federoff IRmiftah_wahyudi100% (1)
- Dignity and SufferingDocument5 paginiDignity and SufferingSilvia MihaelaÎncă nu există evaluări
- History of Hospitals in Craiova During the 19th CenturyDocument10 paginiHistory of Hospitals in Craiova During the 19th CenturySilvia MihaelaÎncă nu există evaluări
- Dignity and SufferingDocument5 paginiDignity and SufferingSilvia MihaelaÎncă nu există evaluări
- A Dissociation Between Similarity EffectsDocument9 paginiA Dissociation Between Similarity EffectsSilvia MihaelaÎncă nu există evaluări
- Dignity and SufferingDocument5 paginiDignity and SufferingSilvia MihaelaÎncă nu există evaluări
- Entitled To Sex Attitudes of Sexual OffendersDocument16 paginiEntitled To Sex Attitudes of Sexual OffendersSilvia MihaelaÎncă nu există evaluări
- 99Document5 pagini99Rafael RamosÎncă nu există evaluări
- A Psychological Profile of A Serial KillerDocument18 paginiA Psychological Profile of A Serial KillerNicoleivgÎncă nu există evaluări
- ESTD Newsletter Volume3 Number 6 March 2014Document31 paginiESTD Newsletter Volume3 Number 6 March 2014Silvia MihaelaÎncă nu există evaluări
- History Docu PhotoDocument5 paginiHistory Docu PhotoSilvia MihaelaÎncă nu există evaluări
- A Dissociation Between Similarity Effects in Episodic Face RecognitionDocument9 paginiA Dissociation Between Similarity Effects in Episodic Face RecognitionSilvia Mihaela100% (1)
- Behavioural Characteristics of RapistsDocument13 paginiBehavioural Characteristics of Rapistsluque_12Încă nu există evaluări
- Photoshop TutorialDocument9 paginiPhotoshop TutorialSilvia MihaelaÎncă nu există evaluări
- Humiliation and ViolnceDocument9 paginiHumiliation and ViolnceSilvia MihaelaÎncă nu există evaluări
- Norton Healthcare News: February 2010Document12 paginiNorton Healthcare News: February 2010Norton HealthcareÎncă nu există evaluări
- DreamsDocument52 paginiDreamsNill SalunkeÎncă nu există evaluări
- Grodberg Et Al., 2015 Diagnostico Observacional Simplificado en AutismoDocument7 paginiGrodberg Et Al., 2015 Diagnostico Observacional Simplificado en AutismoRicardo Jose De LeonÎncă nu există evaluări
- Psychiatric Nursing PDFDocument50 paginiPsychiatric Nursing PDFRalph Lorenz Avila AquinoÎncă nu există evaluări
- Clozapine Drug StudyDocument2 paginiClozapine Drug Studymilkv100% (8)
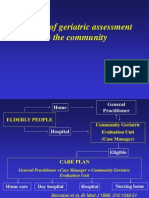
- The Use of Geriatric Assessment in The CommunityDocument16 paginiThe Use of Geriatric Assessment in The Communityhendra2darmawanÎncă nu există evaluări
- Hawthorn (COC) - Verified Class Action Complaint 4-28-23Document51 paginiHawthorn (COC) - Verified Class Action Complaint 4-28-23Morgan RussÎncă nu există evaluări
- UntitledDocument32 paginiUntitledAsmaa AyadÎncă nu există evaluări
- Murawski 2009Document6 paginiMurawski 2009Sofia Valeria MonrealÎncă nu există evaluări
- Sample Intake PaperDocument5 paginiSample Intake PaperSinthia RahmanÎncă nu există evaluări
- Unit 4 Worksheet-1Document4 paginiUnit 4 Worksheet-1Jacie Phillips100% (3)
- Document PDFDocument277 paginiDocument PDFMadhu SudhanÎncă nu există evaluări
- 13 Flashbacks and HPPDDocument7 pagini13 Flashbacks and HPPDRyan MalsÎncă nu există evaluări
- OCD - Thinking Bad ThoughtsDocument5 paginiOCD - Thinking Bad Thoughtshindu2012Încă nu există evaluări
- Treating Self-Harm in Children and Adolescents: Linked ArticlesDocument5 paginiTreating Self-Harm in Children and Adolescents: Linked ArticlesprabhaÎncă nu există evaluări
- Tyrer 2018 - HipocondriaDocument8 paginiTyrer 2018 - HipocondriaBeltraoNayaraÎncă nu există evaluări
- DSM-IV Adult ADHD Symptom Checklist-Self Report Version # 6182Document1 paginăDSM-IV Adult ADHD Symptom Checklist-Self Report Version # 6182Chris0% (1)
- Liste Des Tests - TestothèqueDocument26 paginiListe Des Tests - TestothèqueAbir DocÎncă nu există evaluări
- Psychiatric NursingDocument2 paginiPsychiatric NursingRn nadeenÎncă nu există evaluări
- Essay 2 Working With Crisis and Trauma Draft 1 DO THHIS ONE Auto Saved) Auto Saved) Auto Saved)Document26 paginiEssay 2 Working With Crisis and Trauma Draft 1 DO THHIS ONE Auto Saved) Auto Saved) Auto Saved)Emily SummersÎncă nu există evaluări
- Enright, Liz Coffey, Sage (Ed.) - 'Sweaty Palms - The Anthology About Anxiety'. 2016 PDFDocument384 paginiEnright, Liz Coffey, Sage (Ed.) - 'Sweaty Palms - The Anthology About Anxiety'. 2016 PDFThasÎncă nu există evaluări
- Constantino Decisionagainst Yong LiDocument19 paginiConstantino Decisionagainst Yong Liyong01776Încă nu există evaluări
- 27.çocuk KongreDocument354 pagini27.çocuk KongreogulcanÎncă nu există evaluări
- Depression ResearchDocument12 paginiDepression ResearchIsaiah Diunne Magat Semilla50% (2)
- Doh Philippines Ao-2016-0042Document111 paginiDoh Philippines Ao-2016-0042Keith Aquino100% (1)
- FamilyDocument3 paginiFamilymoses machiraÎncă nu există evaluări
- Anxiety AlgorithmDocument4 paginiAnxiety AlgorithmrizkyswandaruÎncă nu există evaluări
- AngerDocument27 paginiAngerikram ullah khanÎncă nu există evaluări
- The Future of Play TherapyDocument9 paginiThe Future of Play TherapyS EÎncă nu există evaluări
- Healing Through Architecture: A Rehabilitation Center for SchizophreniaDocument16 paginiHealing Through Architecture: A Rehabilitation Center for SchizophreniaNaveen ReddyÎncă nu există evaluări
- Summary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisDe la EverandSummary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (2)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipDe la EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipEvaluare: 4.5 din 5 stele4.5/5 (1135)
- The House Mate: A gripping psychological thriller you won't be able to put downDe la EverandThe House Mate: A gripping psychological thriller you won't be able to put downEvaluare: 4 din 5 stele4/5 (126)
- Summary of The Art of Seduction by Robert GreeneDe la EverandSummary of The Art of Seduction by Robert GreeneEvaluare: 4 din 5 stele4/5 (46)
- The Bridesmaid: The addictive psychological thriller that everyone is talking aboutDe la EverandThe Bridesmaid: The addictive psychological thriller that everyone is talking aboutEvaluare: 4 din 5 stele4/5 (131)
- For Women Only, Revised and Updated Edition: What You Need to Know About the Inner Lives of MenDe la EverandFor Women Only, Revised and Updated Edition: What You Need to Know About the Inner Lives of MenEvaluare: 4.5 din 5 stele4.5/5 (270)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndDe la EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndÎncă nu există evaluări
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- Make Him BEG for Your Attention: 75 Communication Secrets for Captivating Men to Get the Love and Commitment You DeserveDe la EverandMake Him BEG for Your Attention: 75 Communication Secrets for Captivating Men to Get the Love and Commitment You DeserveEvaluare: 4.5 din 5 stele4.5/5 (219)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedEvaluare: 4 din 5 stele4/5 (11)
- How to Walk into a Room: The Art of Knowing When to Stay and When to Walk AwayDe la EverandHow to Walk into a Room: The Art of Knowing When to Stay and When to Walk AwayEvaluare: 4.5 din 5 stele4.5/5 (5)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerDe la EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerEvaluare: 4.5 din 5 stele4.5/5 (58)
- Queen Bee: A brand new addictive psychological thriller from the author of The BridesmaidDe la EverandQueen Bee: A brand new addictive psychological thriller from the author of The BridesmaidEvaluare: 4 din 5 stele4/5 (132)
- Being Mean: A Memoir of Sexual Abuse and SurvivalDe la EverandBeing Mean: A Memoir of Sexual Abuse and SurvivalEvaluare: 4.5 din 5 stele4.5/5 (55)
- Polysecure: Attachment, Trauma and Consensual NonmonogamyDe la EverandPolysecure: Attachment, Trauma and Consensual NonmonogamyEvaluare: 4.5 din 5 stele4.5/5 (221)
- The Waitress: The gripping, edge-of-your-seat psychological thriller from the bestselling author of The BridesmaidDe la EverandThe Waitress: The gripping, edge-of-your-seat psychological thriller from the bestselling author of The BridesmaidEvaluare: 4 din 5 stele4/5 (65)
- White Dresses: A Memoir of Love and Secrets, Mothers and DaughtersDe la EverandWhite Dresses: A Memoir of Love and Secrets, Mothers and DaughtersEvaluare: 4 din 5 stele4/5 (15)
- My Little Brother: The unputdownable, page-turning psychological thriller from Diane SaxonDe la EverandMy Little Brother: The unputdownable, page-turning psychological thriller from Diane SaxonEvaluare: 4.5 din 5 stele4.5/5 (38)
- The Guilty Wife: A gripping addictive psychological suspense thriller with a twist you won’t see comingDe la EverandThe Guilty Wife: A gripping addictive psychological suspense thriller with a twist you won’t see comingEvaluare: 4 din 5 stele4/5 (71)
- Secure Love: Create a Relationship That Lasts a LifetimeDe la EverandSecure Love: Create a Relationship That Lasts a LifetimeEvaluare: 5 din 5 stele5/5 (18)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingDe la EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingÎncă nu există evaluări
- How to Know a Person: The Art of Seeing Others Deeply and Being Deeply Seen v by David Brooks: key Takeaways, Summary & AnalysisDe la EverandHow to Know a Person: The Art of Seeing Others Deeply and Being Deeply Seen v by David Brooks: key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Never Chase Men Again: 38 Dating Secrets to Get the Guy, Keep Him Interested, and Prevent Dead-End RelationshipsDe la EverandNever Chase Men Again: 38 Dating Secrets to Get the Guy, Keep Him Interested, and Prevent Dead-End RelationshipsEvaluare: 4.5 din 5 stele4.5/5 (387)
- Sharing Too Much: Musings from an Unlikely LifeDe la EverandSharing Too Much: Musings from an Unlikely LifeEvaluare: 4.5 din 5 stele4.5/5 (8)