S-ar putea să vă placă și
- Hellp NormotensivoDocument5 paginiHellp NormotensivoJose Alonso Alcoser ArcilaÎncă nu există evaluări
- Inmunologia de PreeclampsiaDocument11 paginiInmunologia de PreeclampsiaJose Alonso Alcoser ArcilaÎncă nu există evaluări
- Supresion Andrigenica Temprana Vs Tardia en Pacientes Con Nodulos Linfoides Por Cancer de Prostata Luego de Terapia Local, Un Itento CurativoDocument13 paginiSupresion Andrigenica Temprana Vs Tardia en Pacientes Con Nodulos Linfoides Por Cancer de Prostata Luego de Terapia Local, Un Itento CurativoJose Alonso Alcoser ArcilaÎncă nu există evaluări
- 2014 Treatment of Hepatitis CDocument10 pagini2014 Treatment of Hepatitis CYuri Rafael Chiclayo CubasÎncă nu există evaluări
- Sepsis y ShockDocument10 paginiSepsis y ShockJose Alonso Alcoser ArcilaÎncă nu există evaluări
- Guía Europea 2012 ICDocument61 paginiGuía Europea 2012 ICJose Alonso Alcoser ArcilaÎncă nu există evaluări
- JNC VIII-full TextDocument14 paginiJNC VIII-full TextvitauxianaÎncă nu există evaluări
- Insulino Resistencia y SOPDocument50 paginiInsulino Resistencia y SOPJose Alonso Alcoser ArcilaÎncă nu există evaluări
- KillipDocument7 paginiKillipIka Choiriyah LusiatiÎncă nu există evaluări
- Colangiocarcinoma. Actualización, Diagnóstico y Terapia: CholangiocarcinomaDocument9 paginiColangiocarcinoma. Actualización, Diagnóstico y Terapia: CholangiocarcinomaElard Paredes MacedoÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5783)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
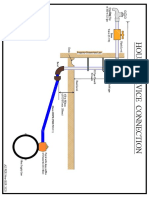
- House Service Connection NEW BSR 2020-1Document1 paginăHouse Service Connection NEW BSR 2020-1Deshraj BairwaÎncă nu există evaluări
- Science Technologyand International RelationsDocument20 paginiScience Technologyand International RelationsMuhammad HussainÎncă nu există evaluări
- Curriculum Vitae of Masilo ModibaDocument11 paginiCurriculum Vitae of Masilo Modibalevy2011Încă nu există evaluări
- Self EducationDocument21 paginiSelf EducationSwami VedatitanandaÎncă nu există evaluări
- A Community School: Research Aspect 2 ReportDocument13 paginiA Community School: Research Aspect 2 ReportMarsha MianÎncă nu există evaluări
- Audit Reveals Optimization Opportunities for Cement Ball Mill SystemDocument19 paginiAudit Reveals Optimization Opportunities for Cement Ball Mill SystemVijay Bhan100% (2)
- ADAMHAND8A4Document11 paginiADAMHAND8A4Elker José Camargo100% (1)
- Application of Operations Research in Banking FinanceDocument13 paginiApplication of Operations Research in Banking FinanceInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Fakeaway - Healthy Home-Cooked Takeaway MealsDocument194 paginiFakeaway - Healthy Home-Cooked Takeaway MealsBiên Nguyễn HữuÎncă nu există evaluări
- Electric Charge: Conservation and Quantization Conductors, Insulators, and Induced ChargesDocument21 paginiElectric Charge: Conservation and Quantization Conductors, Insulators, and Induced ChargesAcadGucciManeÎncă nu există evaluări
- DD Cen TR 10347-2006Document14 paginiDD Cen TR 10347-2006prabagaran88% (8)
- Comp7 - Answer Key - Dec. Exam - 1st SetDocument2 paginiComp7 - Answer Key - Dec. Exam - 1st SetHazel Joy LusellaÎncă nu există evaluări
- Ashrae 62.1-2019Document92 paginiAshrae 62.1-2019Alejandro Castillo100% (16)
- CSS9 TQ PT 3rd4thDocument8 paginiCSS9 TQ PT 3rd4thJevan Hope BaltazarÎncă nu există evaluări
- Surface-Based Transport Model For Mixed-Size Sediment: Peter R. Wilcock, M.ASCE, and Joanna C. CroweDocument9 paginiSurface-Based Transport Model For Mixed-Size Sediment: Peter R. Wilcock, M.ASCE, and Joanna C. CroweEdwinÎncă nu există evaluări
- 02 - AFT - Know Your Pump & System Curves - Part 2ADocument8 pagini02 - AFT - Know Your Pump & System Curves - Part 2AAlfonso José García LagunaÎncă nu există evaluări
- Astm F477-08Document4 paginiAstm F477-08ALARCONISTAÎncă nu există evaluări
- DVRP Newsletter Resilience Vol. 2, Issue 2Document6 paginiDVRP Newsletter Resilience Vol. 2, Issue 2Lucius Doxerie Sr.Încă nu există evaluări
- Improving MV Underground Cable Performance - Experience of TNB MalaysiaDocument4 paginiImproving MV Underground Cable Performance - Experience of TNB Malaysialbk50Încă nu există evaluări
- GPS Navigator: ModelDocument99 paginiGPS Navigator: ModelMain UddinÎncă nu există evaluări
- AIA Design Development Deliverable ListDocument8 paginiAIA Design Development Deliverable Listpeterhwilliams100% (1)
- A Project Report On: "Recreation Club"Document80 paginiA Project Report On: "Recreation Club"Appz100% (2)
- Djoko The Indonesian Mineral Mining Sector Prospects and ChallengesDocument42 paginiDjoko The Indonesian Mineral Mining Sector Prospects and ChallengesUmesh ShanmugamÎncă nu există evaluări
- Assignment IDocument2 paginiAssignment Ivaishnavi priyaÎncă nu există evaluări
- Network 18Document44 paginiNetwork 18Ashok ThakurÎncă nu există evaluări
- Experimental Validation of The BAC Factor Method For Lighting SystemsDocument5 paginiExperimental Validation of The BAC Factor Method For Lighting SystemsJireh AngÎncă nu există evaluări
- AmadeusDocument3 paginiAmadeusCleofe Mae Piñero AseñasÎncă nu există evaluări
- TOEFL Module 1 - ReadingDocument65 paginiTOEFL Module 1 - ReadingImam NurviyantoÎncă nu există evaluări
- Sektion Installation Guide Fy21 Web ADocument16 paginiSektion Installation Guide Fy21 Web AmroliverridleyÎncă nu există evaluări
- Greek MathemaDocument6 paginiGreek MathemaSebastian GhermanÎncă nu există evaluări