S-ar putea să vă placă și
- Unity of Health Through Yogaand Islamic ShalatDocument6 paginiUnity of Health Through Yogaand Islamic ShalatAnonymous SQNcItqXQnÎncă nu există evaluări
- 7903 35982 3 PBDocument9 pagini7903 35982 3 PBEl-yes Yonirazer El-BanjaryÎncă nu există evaluări
- Between the Backbone and the Ribs: Quran on Male Sexual FunctionDocument3 paginiBetween the Backbone and the Ribs: Quran on Male Sexual FunctionAnonymous SQNcItqXQnÎncă nu există evaluări
- Fasting EffectsDocument5 paginiFasting EffectsAnonymous SQNcItqXQnÎncă nu există evaluări
- 01-185.PDF. Shalat Geriatri Pasien #Document4 pagini01-185.PDF. Shalat Geriatri Pasien #Aad IbrahimÎncă nu există evaluări
- Fasting Effects1 PDFDocument4 paginiFasting Effects1 PDFAnonymous SQNcItqXQnÎncă nu există evaluări
- Biomechanical Response of Upper Body Muscles during Salat and Child's PoseDocument4 paginiBiomechanical Response of Upper Body Muscles during Salat and Child's PoseAnonymous SQNcItqXQnÎncă nu există evaluări
- Cardiothoracic TraumaDocument8 paginiCardiothoracic TraumaAnonymous SQNcItqXQnÎncă nu există evaluări
- 6.1 Smart Business Networks - How The Network WinsDocument8 pagini6.1 Smart Business Networks - How The Network WinsAnonymous SQNcItqXQnÎncă nu există evaluări
- Cyber Security Concerns For Emergency ManagementDocument21 paginiCyber Security Concerns For Emergency ManagementAnonymous SQNcItqXQnÎncă nu există evaluări
- Human Genetics and IslamDocument8 paginiHuman Genetics and IslamAnonymous SQNcItqXQnÎncă nu există evaluări
- Qatar Interprofessional Health Council - IPE For QatarDocument9 paginiQatar Interprofessional Health Council - IPE For QatarAnonymous SQNcItqXQnÎncă nu există evaluări
- GI Disorders and CuresDocument19 paginiGI Disorders and CurespjsworldÎncă nu există evaluări
- Puncture Wounds and Mammalian BitesDocument6 paginiPuncture Wounds and Mammalian BitesAnonymous SQNcItqXQnÎncă nu există evaluări
- Glide Well Notes 7Document8 paginiGlide Well Notes 7Amirah SyahirahÎncă nu există evaluări
- Surgery BasicsDocument6 paginiSurgery Basicssharu4291Încă nu există evaluări
- Syria and Assyria Synonyms?Document7 paginiSyria and Assyria Synonyms?marfosdÎncă nu există evaluări
- Leni MardawatiDocument6 paginiLeni MardawatiFeranita AbdurrahmanÎncă nu există evaluări
- PT GARUDA INDONESIA E-TICKET RECEIPT FOR HENRI PERWIRA NEGARADocument2 paginiPT GARUDA INDONESIA E-TICKET RECEIPT FOR HENRI PERWIRA NEGARAAnonymous SQNcItqXQnÎncă nu există evaluări
- Guanabana - Soursop PDFDocument2 paginiGuanabana - Soursop PDFAj GuanzonÎncă nu există evaluări
- Specific Indications in Clinical PracticeDocument58 paginiSpecific Indications in Clinical PracticeOccult Librarian100% (5)
- Charachteristics of A Muslim PhysicianDocument3 paginiCharachteristics of A Muslim PhysicianAnonymous SQNcItqXQnÎncă nu există evaluări
- Efek Bekam1Document2 paginiEfek Bekam1Anonymous SQNcItqXQnÎncă nu există evaluări
- The Syrian Conflict For DummiesDocument17 paginiThe Syrian Conflict For DummiesAnonymous SQNcItqXQnÎncă nu există evaluări
- Guanabana - Soursop PDFDocument2 paginiGuanabana - Soursop PDFAj GuanzonÎncă nu există evaluări
- Khutbah Jumat 2Document5 paginiKhutbah Jumat 2Anonymous SQNcItqXQnÎncă nu există evaluări
- Qadha' Qadar2Document3 paginiQadha' Qadar2Anonymous SQNcItqXQnÎncă nu există evaluări
- From Cell To System, From Mechanism To DiseaseDocument2 paginiFrom Cell To System, From Mechanism To DiseaseAnonymous SQNcItqXQnÎncă nu există evaluări
- Psycho-Spiritual Strategies in Treating Addiction PatientsDocument5 paginiPsycho-Spiritual Strategies in Treating Addiction PatientsAnonymous SQNcItqXQn100% (1)
- Charachteristics of A Muslim PhysicianDocument3 paginiCharachteristics of A Muslim PhysicianAnonymous SQNcItqXQnÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Analgetik Antipiretik AntiinflamasiDocument76 paginiAnalgetik Antipiretik AntiinflamasiranifebÎncă nu există evaluări
- 4a Rota-Vaccine Administration KenyaDocument21 pagini4a Rota-Vaccine Administration KenyaSandraÎncă nu există evaluări
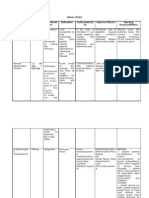
- Drug StudyDocument9 paginiDrug StudyAysaaa DCÎncă nu există evaluări
- CIS Importers ListDocument2 paginiCIS Importers ListAmit SakpalÎncă nu există evaluări
- Daftar Obat-ObatanDocument8 paginiDaftar Obat-Obatanklinik keluargaÎncă nu există evaluări
- Pill Mill-Mori Dalton IndictmentDocument16 paginiPill Mill-Mori Dalton IndictmentSouthern Maryland OnlineÎncă nu există evaluări
- PRELIMSDocument21 paginiPRELIMSPrincess NicoleÎncă nu există evaluări
- Sildenafil Citrate: Sexual DysfunctionDocument8 paginiSildenafil Citrate: Sexual DysfunctionPits MitsÎncă nu există evaluări
- CNS Drugs: Drugs Acting On Central Nervous SystemDocument17 paginiCNS Drugs: Drugs Acting On Central Nervous Systemreza_juÎncă nu există evaluări
- Ondansetron 4Mg Tablets (Ondansetron Hydrochloride) PL 04543/0509 Ondansetron 8Mg Tablets (Ondansetron Hydrochloride) PL 04543/0510Document47 paginiOndansetron 4Mg Tablets (Ondansetron Hydrochloride) PL 04543/0509 Ondansetron 8Mg Tablets (Ondansetron Hydrochloride) PL 04543/0510Santosh VarmaÎncă nu există evaluări
- Cara Efektif Melakukan Stock OpnameDocument126 paginiCara Efektif Melakukan Stock OpnameDita PrimandariÎncă nu există evaluări
- Drug Study ArraDocument5 paginiDrug Study ArraPaul ManaloÎncă nu există evaluări
- Katzung LaxativesDocument6 paginiKatzung LaxativesLonnieAllenVirtudesÎncă nu există evaluări
- Chapter 10Document45 paginiChapter 10Hannah BuquironÎncă nu există evaluări
- BPT Question BankDocument10 paginiBPT Question BankRoydenPTÎncă nu există evaluări
- Daftar Harga HD Juni 2020Document34 paginiDaftar Harga HD Juni 2020Kean KhamidaaÎncă nu există evaluări
- Procto Synalar-N Rectal Cream FormulationDocument2 paginiProcto Synalar-N Rectal Cream FormulationSasho BojadzievÎncă nu există evaluări
- Stok Opname & Pengajuan 09 NovemberDocument24 paginiStok Opname & Pengajuan 09 NovemberAnnisa duaÎncă nu există evaluări
- Format OpnameDocument21 paginiFormat OpnamerestutiyanaÎncă nu există evaluări
- Drug Abuse and Addiction Quiz AnswersDocument10 paginiDrug Abuse and Addiction Quiz AnswersDanyal NadeemÎncă nu există evaluări
- Introduction To PharmacologyDocument50 paginiIntroduction To PharmacologyAbdishakour Hassa.100% (1)
- WHO Pharm 2-2023Document19 paginiWHO Pharm 2-2023Paola Cristini Gama SilvaÎncă nu există evaluări
- Steroids QuizDocument3 paginiSteroids Quizfaqed ilzakiraÎncă nu există evaluări
- Vendedores 01-12-22 ExcelDocument54 paginiVendedores 01-12-22 ExcelDaniel Gonzalez Amaro100% (1)
- Ncma216: BSN 2Nd Year 1St Semester Prelim 2021: Bachelor of Science in Nursing 2YADocument32 paginiNcma216: BSN 2Nd Year 1St Semester Prelim 2021: Bachelor of Science in Nursing 2YAMARIA STEPHANY DELA CRUZ100% (1)
- Panadol Osteo Product InformationDocument5 paginiPanadol Osteo Product Informationsalema2Încă nu există evaluări
- Rle Lectures Medications: Arturo G. Garcia JR RN, MSN, U.S RNDocument33 paginiRle Lectures Medications: Arturo G. Garcia JR RN, MSN, U.S RNMaria Paula Amor GeronimoÎncă nu există evaluări
- Tiaft Drug Concentration Reference TableDocument20 paginiTiaft Drug Concentration Reference TablerodrigoÎncă nu există evaluări
- 10 Rights of Drug Administration With Nursing ImplicationsDocument3 pagini10 Rights of Drug Administration With Nursing ImplicationsJet Bautista100% (6)
- German RemediesDocument2 paginiGerman RemediesbhuvaneshkmrsÎncă nu există evaluări