S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Blueprints Obstetrics and Gynecology 5th Edition MCQDocument30 paginiBlueprints Obstetrics and Gynecology 5th Edition MCQsinglez100% (1)
- Chapter 12Document16 paginiChapter 12Ruthleen May Simeon100% (1)
- Xv. Discharge Plan METHODS - Medication, Exercise, Treatment, Health Teaching, Out-Patient, Diet, Sexuality/SpiritualDocument4 paginiXv. Discharge Plan METHODS - Medication, Exercise, Treatment, Health Teaching, Out-Patient, Diet, Sexuality/SpiritualMichael Bon MargajaÎncă nu există evaluări
- Nursing Care Plan CholecystectomyDocument2 paginiNursing Care Plan Cholecystectomyderic87% (23)
- Kubie, L. (1971) - The Destructive Potential of Humor in PsychotherapyDocument6 paginiKubie, L. (1971) - The Destructive Potential of Humor in PsychotherapyMikaelaMundell100% (1)
- 2020 WHO Global Tuberculosis ReportDocument232 pagini2020 WHO Global Tuberculosis Reportsana shakeelÎncă nu există evaluări
- A Travel Medicine CaseDocument65 paginiA Travel Medicine CaseDiskta W RonicaÎncă nu există evaluări
- Paediatrica Indonesiana: M. Sholeh Kosim, N.P. Noerpramana, Asril Aminullah, Suharyo HadisaputroDocument6 paginiPaediatrica Indonesiana: M. Sholeh Kosim, N.P. Noerpramana, Asril Aminullah, Suharyo HadisaputroDiskta W RonicaÎncă nu există evaluări
- Catatonia, Neuroleptic Malignant Syndrome, and Cotard Syndrome in A 22-Year-Old Woman - A Case ReportDocument3 paginiCatatonia, Neuroleptic Malignant Syndrome, and Cotard Syndrome in A 22-Year-Old Woman - A Case ReportDiskta W RonicaÎncă nu există evaluări
- Diagnosis of Scabies With DermosDocument2 paginiDiagnosis of Scabies With DermosDiskta W RonicaÎncă nu există evaluări
- Diagnosis and Management of Gastroesophageal Reflux Disease (GERD) : An Indian PerspectiveDocument8 paginiDiagnosis and Management of Gastroesophageal Reflux Disease (GERD) : An Indian PerspectiveDiskta W RonicaÎncă nu există evaluări
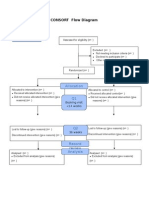
- Additional File 1: CONSORT Flow Diagram: EnrollmentDocument1 paginăAdditional File 1: CONSORT Flow Diagram: EnrollmentDiskta W RonicaÎncă nu există evaluări
- Nursing Management of During Stages of Labor and Delivery UpdatedDocument60 paginiNursing Management of During Stages of Labor and Delivery UpdatedSherlyn Miranda GarcesÎncă nu există evaluări
- CME Trunk, Abdomen, and Pressure Sore ReconstructionDocument15 paginiCME Trunk, Abdomen, and Pressure Sore ReconstructionVeronica TomaselloÎncă nu există evaluări
- Phlebtomy Guidelines and Order of DrawDocument3 paginiPhlebtomy Guidelines and Order of Drawohemgee wowÎncă nu există evaluări
- Malay, Age: 59 Years Old, Date of Admission: 18 August 2009 (CCU), 26 August 2009 (Ward 6B), Date of Clerking: 26 August 2009, Source ofDocument8 paginiMalay, Age: 59 Years Old, Date of Admission: 18 August 2009 (CCU), 26 August 2009 (Ward 6B), Date of Clerking: 26 August 2009, Source ofAiman ArifinÎncă nu există evaluări
- Annisa Fitriani-19.008-THE TASK OF MAKING SENTENCESDocument2 paginiAnnisa Fitriani-19.008-THE TASK OF MAKING SENTENCESAnnisa FitrianiÎncă nu există evaluări
- Is Regenerative Medicine Right For Your Condition?: PRP InjectionsDocument2 paginiIs Regenerative Medicine Right For Your Condition?: PRP InjectionsSamuel AnkomaheneÎncă nu există evaluări
- GAS Turner-Stokes-2009 PDFDocument13 paginiGAS Turner-Stokes-2009 PDFAndrea FloresÎncă nu există evaluări
- Health - WikipediaDocument16 paginiHealth - WikipediakddorÎncă nu există evaluări
- Migrane.20220709015224Document8 paginiMigrane.20220709015224Laharika KatheramallaÎncă nu există evaluări
- Aromatherapy Associates DejnuyoDocument5 paginiAromatherapy Associates Dejnuyobaroqueclothing4269Încă nu există evaluări
- Closer The Client Is To The Origination of Risk, The Higher The Risk For Complications. Sometimes, The TimeDocument3 paginiCloser The Client Is To The Origination of Risk, The Higher The Risk For Complications. Sometimes, The Timeiamlx2100% (1)
- Prof Norhayati RMC KPJUCDocument18 paginiProf Norhayati RMC KPJUCtheskywlkrÎncă nu există evaluări
- Resume Ogechi UkachuDocument3 paginiResume Ogechi UkachuSlahuddin KhanÎncă nu există evaluări
- A Review of Strategies To Decrease The Duration of Indwelling Urethral Catheters and Potentially Reduce The Incidence of Catheter-Associated Urinary Tract Infections - ProQuestDocument10 paginiA Review of Strategies To Decrease The Duration of Indwelling Urethral Catheters and Potentially Reduce The Incidence of Catheter-Associated Urinary Tract Infections - ProQuestHelmy HanafiÎncă nu există evaluări
- Thesis OsteopathyDocument6 paginiThesis Osteopathygbv8rcfq100% (1)
- Kesehatan Indonesia. 2016.: Daftar PustakaDocument2 paginiKesehatan Indonesia. 2016.: Daftar PustakaSiti Raudatus SolihahÎncă nu există evaluări
- Cytomegalovirus Infection: Dr. Hendra Purnasidha Bagaswoto, M.SC, Sp.A SMF Anak RSUP Dr. Soeradji Tirtonegoro KlatenDocument40 paginiCytomegalovirus Infection: Dr. Hendra Purnasidha Bagaswoto, M.SC, Sp.A SMF Anak RSUP Dr. Soeradji Tirtonegoro KlatenDonniehh Assassintilldeath NothinglastforeverÎncă nu există evaluări
- Allergy Clinic Policy and ProceduresDocument4 paginiAllergy Clinic Policy and ProceduresMiselonÎncă nu există evaluări
- Per Rectal Bleeding CompiledDocument33 paginiPer Rectal Bleeding CompiledRajhmuniran Kandasamy100% (1)
- Hypertensive Disorders in PregnancyDocument47 paginiHypertensive Disorders in PregnancyBenard ChristianoÎncă nu există evaluări
- GBS Review2Document64 paginiGBS Review2Vladimir BasurtoÎncă nu există evaluări
- Shaping The Future - Recent Advances of 3D Printing in Drug and Heatlhcare PDFDocument15 paginiShaping The Future - Recent Advances of 3D Printing in Drug and Heatlhcare PDFyuvinta kalimsaÎncă nu există evaluări
- Warfarin SodiumDocument3 paginiWarfarin SodiumAndrea Huecas TriaÎncă nu există evaluări
- Residential Treatment Fee Agreement - FarmDocument1 paginăResidential Treatment Fee Agreement - FarmDawn FarmÎncă nu există evaluări