S-ar putea să vă placă și
- Housing Works "What's Your Voting Plan?!" Sheet 2018Document1 paginăHousing Works "What's Your Voting Plan?!" Sheet 2018housingworksÎncă nu există evaluări
- NYC World AIDS Day 2015 Coalition Event SaveTheDate Flyer EnglishDocument1 paginăNYC World AIDS Day 2015 Coalition Event SaveTheDate Flyer EnglishhousingworksÎncă nu există evaluări
- End AIDS NY 2020 Coalition, World AIDS Day 2018 Resources ListingDocument3 paginiEnd AIDS NY 2020 Coalition, World AIDS Day 2018 Resources ListinghousingworksÎncă nu există evaluări
- Housing Works Get Out The Vote, Election Day 2018 Fact SheetDocument1 paginăHousing Works Get Out The Vote, Election Day 2018 Fact SheethousingworksÎncă nu există evaluări
- #ICantBreathe/ Dec. 2014-Jan. 2015 Calls-to-Action Flyer, Housing Works Advocacy ActionsDocument2 pagini#ICantBreathe/ Dec. 2014-Jan. 2015 Calls-to-Action Flyer, Housing Works Advocacy ActionshousingworksÎncă nu există evaluări
- Civil Society and Communities Declaration To End HIV: Human Rights Must Come FirstDocument7 paginiCivil Society and Communities Declaration To End HIV: Human Rights Must Come FirsthousingworksÎncă nu există evaluări
- New York State Ending The AIDS Epidemic Blueprint Summary One-SheetDocument2 paginiNew York State Ending The AIDS Epidemic Blueprint Summary One-SheethousingworksÎncă nu există evaluări
- 2018 NYC LGBT March Route MapDocument1 pagină2018 NYC LGBT March Route MaphousingworksÎncă nu există evaluări
- Housing Works Get Out The Vote Election Day 2017Document1 paginăHousing Works Get Out The Vote Election Day 2017housingworksÎncă nu există evaluări
- Hillary Clinton Agenda and Meeting Notes 5.12.16Document9 paginiHillary Clinton Agenda and Meeting Notes 5.12.16Housing WorksÎncă nu există evaluări
- DOHMH Notes On Gov Exec Budget, 2.8.17Document2 paginiDOHMH Notes On Gov Exec Budget, 2.8.17housingworksÎncă nu există evaluări
- NYC World AIDS Day Coalition Program, 12-1-14, Harlem's World Famous ApolloDocument4 paginiNYC World AIDS Day Coalition Program, 12-1-14, Harlem's World Famous ApollohousingworksÎncă nu există evaluări
- Housing Works April 2017 Town Hall Call-to-ActionDocument2 paginiHousing Works April 2017 Town Hall Call-to-ActionhousingworksÎncă nu există evaluări
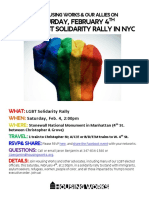
- NYC LGBT Solidarity Rally Flyer For 2 4 17 ExternalDocument1 paginăNYC LGBT Solidarity Rally Flyer For 2 4 17 ExternalhousingworksÎncă nu există evaluări
- May 2016 AIDS Advocates Consensus Policy Paper W EndorsersDocument17 paginiMay 2016 AIDS Advocates Consensus Policy Paper W EndorsershousingworksÎncă nu există evaluări
- AIDS - Free USA 2025 Indiv Sign-On Petition For 2016 Prez Candidates (Download Copy)Document2 paginiAIDS - Free USA 2025 Indiv Sign-On Petition For 2016 Prez Candidates (Download Copy)housingworksÎncă nu există evaluări
- Media Advisory 10.27 AIDS Community Press Conf RE Cuomo Ebola Quarantine FINALDocument1 paginăMedia Advisory 10.27 AIDS Community Press Conf RE Cuomo Ebola Quarantine FINALhousingworksÎncă nu există evaluări
- Housing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, EnglishDocument1 paginăHousing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, EnglishhousingworksÎncă nu există evaluări
- Housing Works Trans Day of Rememberance 2014 Event FlyerDocument1 paginăHousing Works Trans Day of Rememberance 2014 Event FlyerhousingworksÎncă nu există evaluări
- Quarantine - Leadership Letter FINAL 10 26 14Document6 paginiQuarantine - Leadership Letter FINAL 10 26 14housingworksÎncă nu există evaluări
- Nigerian LGBTers Invite To 1/12/15 Veil of Silence Doc ScreeningDocument1 paginăNigerian LGBTers Invite To 1/12/15 Veil of Silence Doc ScreeninghousingworksÎncă nu există evaluări
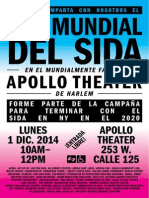
- Housing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, SpanishDocument1 paginăHousing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, SpanishhousingworksÎncă nu există evaluări
- Undetectables Project September 2014 2Document11 paginiUndetectables Project September 2014 2housingworksÎncă nu există evaluări
- Task Force End of AIDS NYS, Opening Remarks, 10.14.14, CKingDocument3 paginiTask Force End of AIDS NYS, Opening Remarks, 10.14.14, CKinghousingworksÎncă nu există evaluări
- Braking AIDS Ride 2014. 9/12-9/14, Cheering Stations GuideDocument1 paginăBraking AIDS Ride 2014. 9/12-9/14, Cheering Stations GuidehousingworksÎncă nu există evaluări
- 2014 IBJ JusticeMakers Award Applications LetterDocument2 pagini2014 IBJ JusticeMakers Award Applications LetterhousingworksÎncă nu există evaluări
- Harrison - Brooklyn ONAP Presentation 8.8.14Document15 paginiHarrison - Brooklyn ONAP Presentation 8.8.14housingworksÎncă nu există evaluări
- O'Connell and Feldman - Manhattan ONAP Presentation 8.7.14Document9 paginiO'Connell and Feldman - Manhattan ONAP Presentation 8.7.14housingworksÎncă nu există evaluări
- Harrison - Brooklyn ONAP Presentation 8.8.14Document15 paginiHarrison - Brooklyn ONAP Presentation 8.8.14housingworksÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Cot DLP Science 6-Simple Machines With AnnotationsDocument9 paginiCot DLP Science 6-Simple Machines With AnnotationsChii Chii100% (21)
- Department of Education: Accomplishment Report On Project Reap (Reading Enhancement Activities For Pupils) S.Y. 2021-2022Document4 paginiDepartment of Education: Accomplishment Report On Project Reap (Reading Enhancement Activities For Pupils) S.Y. 2021-2022Louisse Gayle AntuerpiaÎncă nu există evaluări
- Research into Coma, Esdaile and Sichort States offers New InsightsDocument10 paginiResearch into Coma, Esdaile and Sichort States offers New Insightscoach rismanÎncă nu există evaluări
- Counselling Skills and Techniques GuideDocument29 paginiCounselling Skills and Techniques GuideWanda Lywait100% (1)
- ResearchDocument41 paginiResearchAngel82% (11)
- Sample Chapter - The Ultimate EU Test Book 2013 Administrator (AD) Edition - FreeDocument31 paginiSample Chapter - The Ultimate EU Test Book 2013 Administrator (AD) Edition - FreeAndras Baneth0% (2)
- Communication & Emotional IntelligenceDocument22 paginiCommunication & Emotional IntelligenceRaghuram Bhandari100% (1)
- Definition of Terms: Maed-FilipinoDocument14 paginiDefinition of Terms: Maed-FilipinoMarceline Ruiz0% (1)
- Test Bank in Edcon2: Social Dimension of EducationDocument20 paginiTest Bank in Edcon2: Social Dimension of EducationPaul john caguingÎncă nu există evaluări
- Writing A Concept Paper 190319200413Document24 paginiWriting A Concept Paper 190319200413Julieto Sumatra JrÎncă nu există evaluări
- ADEC - International Community Branch 2016-2017Document23 paginiADEC - International Community Branch 2016-2017Edarabia.comÎncă nu există evaluări
- 10 Sales TechDocument9 pagini10 Sales TechHamdy AlyÎncă nu există evaluări
- Reading and Writing 4 Q: Skills For Success Unit 4 Student Book Answer KeyDocument3 paginiReading and Writing 4 Q: Skills For Success Unit 4 Student Book Answer KeyPoornachandra50% (2)
- OYH Assessment ManualDocument53 paginiOYH Assessment ManualLizPattison9275% (12)
- Ian Angel B. Osnan BECED III Ece 13: Science in Early Childhood Education Faculty: Ms. Dachel LaderaDocument4 paginiIan Angel B. Osnan BECED III Ece 13: Science in Early Childhood Education Faculty: Ms. Dachel LaderaWowie OsnanÎncă nu există evaluări
- Math Grade 7 DLL Q2 W1Document3 paginiMath Grade 7 DLL Q2 W1thalia alfaroÎncă nu există evaluări
- Develop Competency Based Learning MaterialsDocument33 paginiDevelop Competency Based Learning MaterialsEm Boquiren Carreon0% (1)
- Leiter-3 Manual P 46 Corrected SecondsDocument1 paginăLeiter-3 Manual P 46 Corrected SecondsDidenko MarinaÎncă nu există evaluări
- MonologuesDocument7 paginiMonologuesJiggy Derek Mercado0% (2)
- How To Lift Depression Quickly and SafelyDocument4 paginiHow To Lift Depression Quickly and SafelyHuman Givens Publishing Official50% (2)
- Teacher Interview ResponseDocument6 paginiTeacher Interview Responseapi-163091177Încă nu există evaluări
- Patient Centred Leadership in PracticeDocument11 paginiPatient Centred Leadership in Practicerafskall100% (1)
- Aleppo SyriaDocument3 paginiAleppo SyriaKimÎncă nu există evaluări
- New TermDocument97 paginiNew TermEthan PhilipÎncă nu există evaluări
- MAPEH G08 1st Periodical TestDocument3 paginiMAPEH G08 1st Periodical TestDana Reyes100% (2)
- Hello LoveDocument7 paginiHello LoveKrisTin Magbanua Jocson100% (3)
- Teacher Talk and Learner TalkDocument9 paginiTeacher Talk and Learner TalkWong Choy WanÎncă nu există evaluări
- Math 4 Week 6Document10 paginiMath 4 Week 6Julie Ann UrsulumÎncă nu există evaluări
- Patient Safety and Quality Care MovementDocument9 paginiPatient Safety and Quality Care Movementapi-300362983Încă nu există evaluări
- Ratan Tata and His Enterprising SkillsDocument10 paginiRatan Tata and His Enterprising Skillsstarbb100% (1)