S-ar putea să vă placă și
- Imaging Techniques in Glaucoma: Presenter: Dr. Rujuta Moderator: Dr. Rita DhamankarDocument54 paginiImaging Techniques in Glaucoma: Presenter: Dr. Rujuta Moderator: Dr. Rita Dhamankardrvishalkulkarni2007Încă nu există evaluări
- Fast Multispectral Imaging by Spatial Pixel-Binning and Spectral UnmixingDocument7 paginiFast Multispectral Imaging by Spatial Pixel-Binning and Spectral UnmixingRaj VelÎncă nu există evaluări
- OCT Guide To Interpreting PDFDocument98 paginiOCT Guide To Interpreting PDFBrit Lee100% (2)
- Imaging of Glaucoma DiagnosisDocument74 paginiImaging of Glaucoma Diagnosisabiraham zigaleÎncă nu există evaluări
- Braken Hoff 1986Document10 paginiBraken Hoff 1986Annisa HayatiÎncă nu există evaluări
- Depth Enhancement in Spectral Domain Optical Coherence Tomography Using BidirectionalDocument10 paginiDepth Enhancement in Spectral Domain Optical Coherence Tomography Using BidirectionalNareshÎncă nu există evaluări
- Automated 3-D Region-Based Volumetric Estimation of Optic Disc Swelling in Papilledema Using Spectral-Domain Optical Coherence TomographyDocument8 paginiAutomated 3-D Region-Based Volumetric Estimation of Optic Disc Swelling in Papilledema Using Spectral-Domain Optical Coherence TomographyKalo RafinÎncă nu există evaluări
- CBCT in Endodontics: Presented By: DR - Saloni PG Student Dept. of Cons and EndoDocument83 paginiCBCT in Endodontics: Presented By: DR - Saloni PG Student Dept. of Cons and Endosaloni singhÎncă nu există evaluări
- Pubmed Thesis Topics in OphthalmologyDocument5 paginiPubmed Thesis Topics in Ophthalmologyheidiowensspringfield100% (2)
- What Is Cone-Beam CT and How Does It WorkDocument24 paginiWhat Is Cone-Beam CT and How Does It Workosama nasserÎncă nu există evaluări
- Endoscopic 2D Particle Image Velocimetry (PIV) Ow Field Measurements in IC EnginesDocument9 paginiEndoscopic 2D Particle Image Velocimetry (PIV) Ow Field Measurements in IC EnginesSantiago Cano ZapataÎncă nu există evaluări
- Clinical Use and Research Applications of Heidelberg Retinal Angiography and Spectral-Domain Optical Coherence Tomography - A ReviewDocument14 paginiClinical Use and Research Applications of Heidelberg Retinal Angiography and Spectral-Domain Optical Coherence Tomography - A ReviewMashhoor AlfayezÎncă nu există evaluări
- Thesis Topics in Ophthalmology in AiimsDocument5 paginiThesis Topics in Ophthalmology in AiimsBuyCollegePaperOnlineUK100% (1)
- OCT Dynamic-Focusing Microscope Objective For Optical Coherence Tomographyesign 1Document5 paginiOCT Dynamic-Focusing Microscope Objective For Optical Coherence Tomographyesign 1Kumarivalli KannuÎncă nu există evaluări
- The Basics of Maxillofacial Cone Beam Computed Tomography: Allan G. Farman and William C. ScarfeDocument12 paginiThe Basics of Maxillofacial Cone Beam Computed Tomography: Allan G. Farman and William C. ScarfeMANUELA GUTIERREZ MESAÎncă nu există evaluări
- Radio Digital 1Document6 paginiRadio Digital 1Lucy Esther Calvo PerniaÎncă nu există evaluări
- OPD-Scan III: Refractive Power / Corneal AnalyzerDocument6 paginiOPD-Scan III: Refractive Power / Corneal AnalyzerFreeÎncă nu există evaluări
- Ol 38 16 3103Document4 paginiOl 38 16 3103Aswin KumarÎncă nu există evaluări
- Thickness Obtained by Software Image Normative Data of Outer Photoreceptor LayerDocument7 paginiThickness Obtained by Software Image Normative Data of Outer Photoreceptor LayerAzuleslindoÎncă nu există evaluări
- 2012 MotaghiannezamDocument12 pagini2012 MotaghiannezamTim WeberÎncă nu există evaluări
- Digital Mammography RCNADocument14 paginiDigital Mammography RCNADr PiyushÎncă nu există evaluări
- An Intelligent Active Range Sensor For Vehicle Guidance: System OverviewDocument8 paginiAn Intelligent Active Range Sensor For Vehicle Guidance: System OverviewUtsav V ByndoorÎncă nu există evaluări
- Cornealtopographybysuraj 160507151045Document112 paginiCornealtopographybysuraj 160507151045Ridho HariyadiÎncă nu există evaluări
- s12886 017 0419 1Document8 paginis12886 017 0419 1Madhu C KÎncă nu există evaluări
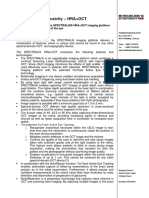
- Certificate of Exclusivity - HRA + OCT EnglishDocument4 paginiCertificate of Exclusivity - HRA + OCT EnglishagmÎncă nu există evaluări
- Recent Advances in Oral Maxillofacial RadiologyDocument98 paginiRecent Advances in Oral Maxillofacial RadiologySijal NiraulaÎncă nu există evaluări
- Anterior Chamber Angle Imaging With Optical Coherence TomographyDocument7 paginiAnterior Chamber Angle Imaging With Optical Coherence TomographySouvik BanerjeeÎncă nu există evaluări
- Sirius ZHeidariMMohammadpourDocument82 paginiSirius ZHeidariMMohammadpourSyamerra YapÎncă nu există evaluări
- CBCT in EndodonticsDocument133 paginiCBCT in EndodonticsAnciya Nazar100% (6)
- A Human-Computer Interface Design Using Automatic Gaze TrackingDocument4 paginiA Human-Computer Interface Design Using Automatic Gaze TrackingBinay PoudelÎncă nu există evaluări
- A Comparison of 18 Different X-Ray Detectors Currently UsedDocument5 paginiA Comparison of 18 Different X-Ray Detectors Currently UsedpnogrlÎncă nu există evaluări
- 1112CRSTEuro Cs VinciguerraDocument3 pagini1112CRSTEuro Cs VinciguerraR Andres Plaza ZÎncă nu există evaluări
- Real-Time Volumetric Microscopy of in Vivo Dynamics and Large-Scale Samples With SCAPE 2.0Document15 paginiReal-Time Volumetric Microscopy of in Vivo Dynamics and Large-Scale Samples With SCAPE 2.0Honghai LiuÎncă nu există evaluări
- Journal Update 2Document6 paginiJournal Update 2Pradipta Hadyan AldiostaÎncă nu există evaluări
- The Impact of Focal Spot Size On Clinical ImagesDocument11 paginiThe Impact of Focal Spot Size On Clinical ImagesSOHON SINHA MAHAPATRAÎncă nu există evaluări
- Young-Sik Ghim KRISSDocument12 paginiYoung-Sik Ghim KRISSشہریار شمسیÎncă nu există evaluări
- Single Photon Emission Computed TomographyDocument15 paginiSingle Photon Emission Computed TomographyChris HartoyoÎncă nu există evaluări
- Fast 5DOF Needle Tracking in iOCTDocument10 paginiFast 5DOF Needle Tracking in iOCTxuedunÎncă nu există evaluări
- Chapter 17 Photokeratos PDFDocument45 paginiChapter 17 Photokeratos PDFfakenameÎncă nu există evaluări
- Three-Dimensional Particle Image Velocimetry: Experimental Error Analysis of A Digital Angular Stereoscopic SystemDocument11 paginiThree-Dimensional Particle Image Velocimetry: Experimental Error Analysis of A Digital Angular Stereoscopic Systemsamik4uÎncă nu există evaluări
- Clinical: Clinical Applications of Cone-Beam Computed Tomography in Dental PracticeDocument6 paginiClinical: Clinical Applications of Cone-Beam Computed Tomography in Dental PracticeNaro HassanÎncă nu există evaluări
- l28 Isi P Bozomitu 2015 Siitme p161Document4 paginil28 Isi P Bozomitu 2015 Siitme p161Doru IrimescuÎncă nu există evaluări
- Use of Confocal Laser Scanning Microscopy (CLSM) For Depthwise Resolved Microscale-Particle Image Velocimetry (m-PIV)Document16 paginiUse of Confocal Laser Scanning Microscopy (CLSM) For Depthwise Resolved Microscale-Particle Image Velocimetry (m-PIV)Cristina PetcuÎncă nu există evaluări
- Imaging in Periodontics PerioDocument49 paginiImaging in Periodontics PerioFourthMolar.comÎncă nu există evaluări
- Image Mosaicing and Real-Time Imaging With Mems Based Handheld Confocal MicroscopeDocument4 paginiImage Mosaicing and Real-Time Imaging With Mems Based Handheld Confocal MicroscopeLuthfan FauzanÎncă nu există evaluări
- The Value of Stereoscopic Optic Disc Photography: An Update On Imaging Techniques and ReliabilityDocument3 paginiThe Value of Stereoscopic Optic Disc Photography: An Update On Imaging Techniques and Reliabilitypqwoeifjpakou134Încă nu există evaluări
- A Theory of Single-Viewpoint Catadioptric Image FormationDocument22 paginiA Theory of Single-Viewpoint Catadioptric Image FormationRajat AggarwalÎncă nu există evaluări
- Computed Radiography Image Artifacts RevisitedDocument11 paginiComputed Radiography Image Artifacts RevisitedsiminithinÎncă nu există evaluări
- Unit 4 MIT Notes SendDocument32 paginiUnit 4 MIT Notes SendEr Amit VermaÎncă nu există evaluări
- Opd - Scan Ii PDFDocument6 paginiOpd - Scan Ii PDFDfhos Oftalmo ServiceÎncă nu există evaluări
- Industrial X-Ray Computed TomographyDe la EverandIndustrial X-Ray Computed TomographySimone CarmignatoÎncă nu există evaluări
- An Integrated Imaging Sensor For Aberration-Corrected 3D PhotographyDocument26 paginiAn Integrated Imaging Sensor For Aberration-Corrected 3D PhotographyKFSwÎncă nu există evaluări
- Inverted Research Microscope ECLIPSE TiDocument32 paginiInverted Research Microscope ECLIPSE TiHamdi SeverÎncă nu există evaluări
- Boe 13 1 65Document17 paginiBoe 13 1 65Rajesh KrishananÎncă nu există evaluări
- Makalah CR DR Dan CT ScanDocument11 paginiMakalah CR DR Dan CT ScanRenolia WidyaningrumÎncă nu există evaluări
- Estimating Velocity of Nailfold Vessels Flow Using Improvised Deconvolution AlgorithmDocument6 paginiEstimating Velocity of Nailfold Vessels Flow Using Improvised Deconvolution AlgorithmIJERDÎncă nu există evaluări
- Artroscopia - PrincipiiDocument24 paginiArtroscopia - PrincipiiMyhay CretzuÎncă nu există evaluări
- LCD SLMDocument9 paginiLCD SLMVipin_Kumar_5649Încă nu există evaluări
- Wang2011 (Sistema Compacto)Document13 paginiWang2011 (Sistema Compacto)Laura PerozaÎncă nu există evaluări
- High-Resolution Imaging Ellipsometer: Qiwen Zhan and James R. LegerDocument8 paginiHigh-Resolution Imaging Ellipsometer: Qiwen Zhan and James R. LegergitarcinayiÎncă nu există evaluări
- What Is NNTDocument8 paginiWhat Is NNTSaraRosa1992Încă nu există evaluări
- AmblyopiaDocument10 paginiAmblyopiaSaraRosa1992Încă nu există evaluări
- Phrasal VerbsDocument6 paginiPhrasal VerbsJulian96% (23)
- Phrasal VerbsDocument6 paginiPhrasal VerbsJulian96% (23)
- 50 Common English Phrasal Verbs PDFDocument54 pagini50 Common English Phrasal Verbs PDFPapitch Do DuneÎncă nu există evaluări
- Chap.1. Brief HX & X-Ray ProductionDocument42 paginiChap.1. Brief HX & X-Ray ProductiongetemeselewÎncă nu există evaluări
- Study Material: Free Master Class SeriesDocument21 paginiStudy Material: Free Master Class SeriesTinku SinglaÎncă nu există evaluări
- Introduction of Optical Networking 2.0Document28 paginiIntroduction of Optical Networking 2.0halimabiÎncă nu există evaluări
- Optica-Dual-Comb SpectrosDocument13 paginiOptica-Dual-Comb SpectrosYe FengÎncă nu există evaluări
- Superconductivity & Optical FibersDocument17 paginiSuperconductivity & Optical FibersMahesh Lohith K.SÎncă nu există evaluări
- Physical Science Q4 Week 5 v2Document21 paginiPhysical Science Q4 Week 5 v2Jojie Sumayang-Golisao100% (1)
- Lecture-5 (Introduction To Outdoor Lighting)Document35 paginiLecture-5 (Introduction To Outdoor Lighting)architectneha614Încă nu există evaluări
- Penguin Energy ProjectDocument11 paginiPenguin Energy Projectamy_k_spearsÎncă nu există evaluări
- Bio Lab ManualDocument56 paginiBio Lab ManualAkash JainÎncă nu există evaluări
- Bifocal Add: Image Jump and Image Displacement: Basic Optics, Chapter 24Document45 paginiBifocal Add: Image Jump and Image Displacement: Basic Optics, Chapter 24PAM ALVARADOÎncă nu există evaluări
- Label Free Super Resolution MicrosDocument498 paginiLabel Free Super Resolution Micros1retuderaÎncă nu există evaluări
- IB PH SL Waves NotesDocument13 paginiIB PH SL Waves NotesT-girlÎncă nu există evaluări
- Microlab NotesDocument4 paginiMicrolab NotesSamantha Nicole S. GaleraÎncă nu există evaluări
- Particle Image Velocimetry (PIV) - Fundamentals & ApplicationsDocument64 paginiParticle Image Velocimetry (PIV) - Fundamentals & ApplicationsFSBollÎncă nu există evaluări
- PresentationDocument38 paginiPresentationAnonymous C09uQydeB100% (1)
- Testing: Performance For Precision 500D Classical R/F SystemDocument25 paginiTesting: Performance For Precision 500D Classical R/F SystemIzah NasirÎncă nu există evaluări
- Electromagnetic Wave Theory: Andre Marie Ampere (1775-1836) in 1820 Finds That Wires CarryingDocument2 paginiElectromagnetic Wave Theory: Andre Marie Ampere (1775-1836) in 1820 Finds That Wires CarryingsarahÎncă nu există evaluări
- Testing of Space Solar Cells & Solar Arrays For Space ApplicationsDocument8 paginiTesting of Space Solar Cells & Solar Arrays For Space ApplicationsJohn Vivian Prashant jp7vivianÎncă nu există evaluări
- SG-05 Safety Guideline For Illumination at WorkplaceDocument5 paginiSG-05 Safety Guideline For Illumination at Workplacetariq1987Încă nu există evaluări
- Pulsed and Continuous Shortwave TherapyDocument29 paginiPulsed and Continuous Shortwave TherapyJames ChiaÎncă nu există evaluări
- 2.1 Fiber Dispersion: Chapter 2: Optical Fiber Characteristics and System ConfigurationsDocument23 pagini2.1 Fiber Dispersion: Chapter 2: Optical Fiber Characteristics and System ConfigurationsSaurav KauraÎncă nu există evaluări
- Materials Science Questions and AnswersDocument7 paginiMaterials Science Questions and Answersد.حاتممرقهÎncă nu există evaluări
- Optct 2022Document15 paginiOptct 2022ajaykumarÎncă nu există evaluări
- Iit Chemistry: EnthuseDocument150 paginiIit Chemistry: EnthuseKushagra PandeyÎncă nu există evaluări
- EE420 SyllabusDocument1 paginăEE420 Syllabussal1980Încă nu există evaluări
- SiteDocument6 paginiSiteMikeÎncă nu există evaluări
- Radiation Production and Characteristics Lecture2021 22Document188 paginiRadiation Production and Characteristics Lecture2021 22Lei ClamorÎncă nu există evaluări
- Antenna Theory & Propagation EC-604A SL No. Slot Duration Module/topic 1 Day 1 1 HourDocument1 paginăAntenna Theory & Propagation EC-604A SL No. Slot Duration Module/topic 1 Day 1 1 HouraparnaÎncă nu există evaluări
- Technical Data Sheet APXV86-909014-C: RFS The Clear Choice ™ APXV86-909014-C Print Date: 09.10.2008Document3 paginiTechnical Data Sheet APXV86-909014-C: RFS The Clear Choice ™ APXV86-909014-C Print Date: 09.10.2008Lenin RamirezÎncă nu există evaluări
- Physics 1230: Light and Color: - Topic 4Document35 paginiPhysics 1230: Light and Color: - Topic 4nidharshanÎncă nu există evaluări