S-ar putea să vă placă și
- Future AncestorsDocument44 paginiFuture AncestorsAlex100% (1)
- (G. Lakshmi Narasaiah) Finite Element Analysis PDFDocument349 pagini(G. Lakshmi Narasaiah) Finite Element Analysis PDFmoljaime1326Încă nu există evaluări
- ST 36Document4 paginiST 36ray72roÎncă nu există evaluări
- The Dry Bulk Management StandardDocument18 paginiThe Dry Bulk Management Standardamu_more44100% (1)
- Killer Kohler Part I IDocument17 paginiKiller Kohler Part I Irusyn100% (1)
- Lower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANDocument3 paginiLower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANHadi FirmansyahÎncă nu există evaluări
- Factors Affecting Physical FitnessDocument7 paginiFactors Affecting Physical FitnessMary Joy Escanillas Gallardo100% (2)
- Aluminium Alloy - Wikipedia, The Free EncyclopediaDocument12 paginiAluminium Alloy - Wikipedia, The Free EncyclopediaAshishJoshi100% (1)
- Overall Method StatementDocument33 paginiOverall Method Statementsaranga100% (1)
- The Joy Luck Club Book 1Document12 paginiThe Joy Luck Club Book 1loronalicelÎncă nu există evaluări
- Prawn ProcessingDocument21 paginiPrawn ProcessingKrishnaÎncă nu există evaluări
- Jurnal Ilham Erry FixDocument21 paginiJurnal Ilham Erry FixIlham Tri HasdiantonoÎncă nu există evaluări
- Biomedicines 10 02105Document16 paginiBiomedicines 10 02105Fatimah AssagafÎncă nu există evaluări
- Foreign Bodies in Aerodigestive Tract A Clinical Review of 109 Patients - July - 2020 - 6161115370 - 0822664Document3 paginiForeign Bodies in Aerodigestive Tract A Clinical Review of 109 Patients - July - 2020 - 6161115370 - 0822664Luis GallegosÎncă nu există evaluări
- Drug Allergy Clinical Characteristics in PediatricsDocument5 paginiDrug Allergy Clinical Characteristics in PediatricsnadyaÎncă nu există evaluări
- Health20120100002 44132100Document5 paginiHealth20120100002 44132100Gautam BhallaÎncă nu există evaluări
- JurnalDocument21 paginiJurnalBhakti Fadzilah NÎncă nu există evaluări
- Late-Presenting Congenital Diaphragmatic HerniaDocument5 paginiLate-Presenting Congenital Diaphragmatic HerniaDara Dasawulansari SyamsuriÎncă nu există evaluări
- Referensi Dari Saya No 8Document7 paginiReferensi Dari Saya No 8Kalsum MbÎncă nu există evaluări
- Discoid Lupus Erythematosus: A Profile: Original ArticleDocument4 paginiDiscoid Lupus Erythematosus: A Profile: Original ArticleAngelin LigiantoÎncă nu există evaluări
- Research ArticleDocument10 paginiResearch ArticlePratama Imanuel RawungÎncă nu există evaluări
- Pattern of ThyroidDocument6 paginiPattern of ThyroidUmaieyaal AnnarajahÎncă nu există evaluări
- Clinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenDocument4 paginiClinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenNurul Huda KowitaÎncă nu există evaluări
- Causes and Treatment Outcomes of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in 82 Adult PatientsDocument8 paginiCauses and Treatment Outcomes of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in 82 Adult PatientschechenoveliaÎncă nu există evaluări
- Right-Sided Colonic Diverticulitis: Clinical Features, Sonographic Appearances, and ManagementDocument7 paginiRight-Sided Colonic Diverticulitis: Clinical Features, Sonographic Appearances, and ManagementgailÎncă nu există evaluări
- SSJ ConvertDocument8 paginiSSJ ConvertHarryPascaRullianÎncă nu există evaluări
- Assessment of T Regulatory Cells in Egyptian Pat - 2021 - Journal of Radiation RDocument8 paginiAssessment of T Regulatory Cells in Egyptian Pat - 2021 - Journal of Radiation REga DuandiniÎncă nu există evaluări
- Jamadermatology Kridin 2021 Oi 210045 1634154542.6481Document9 paginiJamadermatology Kridin 2021 Oi 210045 1634154542.6481Nandha KumarÎncă nu există evaluări
- Risk Factor TaiwanDocument5 paginiRisk Factor TaiwanMira ApriliaÎncă nu există evaluări
- Das 2021Document7 paginiDas 2021Oana Alexandra PetreÎncă nu există evaluări
- Hyper Tiro IdDocument5 paginiHyper Tiro Idkonstantin balabalaÎncă nu există evaluări
- Leprosy in PediatricDocument5 paginiLeprosy in PediatricYusuf Budi HermawanÎncă nu există evaluări
- Acute Cholecystitis: From ER To Surgery: Riginal RticleDocument5 paginiAcute Cholecystitis: From ER To Surgery: Riginal RticleKrystel Joy AuroÎncă nu există evaluări
- Original Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearsDocument6 paginiOriginal Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearssyalalaaalalaaaÎncă nu există evaluări
- WJG 18 4335Document7 paginiWJG 18 4335aalmadasalazarÎncă nu există evaluări
- Kasus 2 Nomor 4Document31 paginiKasus 2 Nomor 4meutia salsabilaÎncă nu există evaluări
- CD 34Document16 paginiCD 34rovia achmad .Încă nu există evaluări
- Kasus 2 Nomor 4Document31 paginiKasus 2 Nomor 4meutia salsabilaÎncă nu există evaluări
- Acute Rheumatic Fever Clinical Profile in Children in Western UkraineDocument5 paginiAcute Rheumatic Fever Clinical Profile in Children in Western UkraineraniaulfahÎncă nu există evaluări
- Or3 PDFDocument5 paginiOr3 PDFAkshay PatilÎncă nu există evaluări
- Rheumatology 2008Document3 paginiRheumatology 2008Thelma Cantillo RochaÎncă nu există evaluări
- Primary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologyDocument6 paginiPrimary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologymiÎncă nu există evaluări
- Rekam Anusha Et Al.Document3 paginiRekam Anusha Et Al.International Journal of Clinical and Biomedical Research (IJCBR)Încă nu există evaluări
- J Oraloncology 2021 105462Document7 paginiJ Oraloncology 2021 105462Maria Isabela GueburÎncă nu există evaluări
- Clinical Outcome in Children With Chronic Recurrent Multifocal OsteomyelitisDocument4 paginiClinical Outcome in Children With Chronic Recurrent Multifocal OsteomyelitisJiwo SaciladhÎncă nu există evaluări
- tmp57C2 TMPDocument7 paginitmp57C2 TMPFrontiersÎncă nu există evaluări
- Profile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyDocument6 paginiProfile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyRose ParkÎncă nu există evaluări
- Journal Siklus Anak 5Document5 paginiJournal Siklus Anak 5dwi-148502Încă nu există evaluări
- 3sharayu EtalDocument4 pagini3sharayu EtaleditorijmrhsÎncă nu există evaluări
- Original ArticleDocument4 paginiOriginal ArticleGoto LaluÎncă nu există evaluări
- Dermatological Signs in Wilson's DiseaseDocument4 paginiDermatological Signs in Wilson's DiseaseGingerWiseÎncă nu există evaluări
- 664 8537 1 PBDocument5 pagini664 8537 1 PBMICHAEL NUGROHOÎncă nu există evaluări
- Patterns of Skin Disease and Prescribing Trends in Rural India Juno J. Joel, Neethu Jose, Shastry C.SDocument6 paginiPatterns of Skin Disease and Prescribing Trends in Rural India Juno J. Joel, Neethu Jose, Shastry C.SHabibur RahmanÎncă nu există evaluări
- A Clinical and Epidemiological Study On Discoid Lupus ErythematosusDocument7 paginiA Clinical and Epidemiological Study On Discoid Lupus Erythematosusiin sakinah dewiÎncă nu există evaluări
- Jurnal PatogenesisDocument6 paginiJurnal PatogenesisErmiati EmhyÎncă nu există evaluări
- Kundak 2020Document6 paginiKundak 2020Diana DîrzuÎncă nu există evaluări
- Journal Reading - SSJ-TENDocument21 paginiJournal Reading - SSJ-TENReski Nursyifah HusainÎncă nu există evaluări
- Severe Cutaneous Adverse Reactions Related To Systemic AntibioticsDocument9 paginiSevere Cutaneous Adverse Reactions Related To Systemic AntibioticsajithloyolaÎncă nu există evaluări
- 1543-2165-134 6 815 PDFDocument11 pagini1543-2165-134 6 815 PDFmmigod666Încă nu există evaluări
- Aair 2 123Document4 paginiAair 2 123Nandha KumarÎncă nu există evaluări
- 679 1364 1 SMDocument5 pagini679 1364 1 SMRetno ManggalihÎncă nu există evaluări
- Necrotising Soft Tissue Infections: The Effect of Hyperbaric Oxygen On MortalityDocument9 paginiNecrotising Soft Tissue Infections: The Effect of Hyperbaric Oxygen On MortalityTony LeeÎncă nu există evaluări
- Article 370Document5 paginiArticle 370Luis Alfredo LucioÎncă nu există evaluări
- Epidemiology, Incidence, and Prevalence of Neuroendocrine Neoplasms Are There Global DifferencesDocument13 paginiEpidemiology, Incidence, and Prevalence of Neuroendocrine Neoplasms Are There Global DifferencesROSARIO PAZ MILLÁNÎncă nu există evaluări
- Tracheobronchial Foreign Bodies : Presentation and Management in Children and AdultsDocument6 paginiTracheobronchial Foreign Bodies : Presentation and Management in Children and AdultsrizkaayusafitriÎncă nu există evaluări
- Draft2 Review DikitDocument9 paginiDraft2 Review DikitGiza HanifÎncă nu există evaluări
- Artigo 2 - Symptomatic Meckel's Diverticulum in Children - A 12-Year Survey - 2021Document4 paginiArtigo 2 - Symptomatic Meckel's Diverticulum in Children - A 12-Year Survey - 2021Larissa RuthyelyÎncă nu există evaluări
- Clinical Epidemiological Profile of Vitiligo in Children and AdolescentsDocument3 paginiClinical Epidemiological Profile of Vitiligo in Children and AdolescentsKarla KaluaÎncă nu există evaluări
- Acute Generalized Exanthematous Pustulosis: Sima HalevyDocument18 paginiAcute Generalized Exanthematous Pustulosis: Sima HalevyDody PrasetyaÎncă nu există evaluări
- Pubmed-Hydatid Disease in Childhood Revisited Report of An InterestingDocument4 paginiPubmed-Hydatid Disease in Childhood Revisited Report of An InterestingAurelian CârsteaÎncă nu există evaluări
- Medical Journals Year in Body Mods 2012 12-30-12Document24 paginiMedical Journals Year in Body Mods 2012 12-30-12Hadi FirmansyahÎncă nu există evaluări
- Chae Et Al-2015-Journal of Cosmetic DermatologyDocument7 paginiChae Et Al-2015-Journal of Cosmetic DermatologyHadi FirmansyahÎncă nu există evaluări
- Bleomycin in The Treatment of Keloids and Hypertrophic Scars by Multiple Needle PuncturesDocument10 paginiBleomycin in The Treatment of Keloids and Hypertrophic Scars by Multiple Needle PuncturesHadi FirmansyahÎncă nu există evaluări
- 10 5923 J Surgery 20140301 03 PDFDocument4 pagini10 5923 J Surgery 20140301 03 PDFJacobMsangÎncă nu există evaluări
- Medical Journals Year in Body Mods 2012 12-30-12Document24 paginiMedical Journals Year in Body Mods 2012 12-30-12Hadi FirmansyahÎncă nu există evaluări
- Treatment of Keloids and Hypertrophic ScarsDocument9 paginiTreatment of Keloids and Hypertrophic ScarsHadi FirmansyahÎncă nu există evaluări
- Bleomycin and The SkinDocument8 paginiBleomycin and The SkinHadi FirmansyahÎncă nu există evaluări
- White Piedra in A Mother and DaughterDocument3 paginiWhite Piedra in A Mother and DaughterHadi FirmansyahÎncă nu există evaluări
- Wilske B. Epidemiology and Diagnosis of Lyme Borreliosis 2005Document12 paginiWilske B. Epidemiology and Diagnosis of Lyme Borreliosis 2005Hadi FirmansyahÎncă nu există evaluări
- Fatal Metastatic Cutaneous Squamous Cell Carcinoma Evolving From A Localized Verrucous Epidermal NevusDocument11 paginiFatal Metastatic Cutaneous Squamous Cell Carcinoma Evolving From A Localized Verrucous Epidermal NevusHadi FirmansyahÎncă nu există evaluări
- Co-Isolation of Trichosporon Inkin and CandidaDocument8 paginiCo-Isolation of Trichosporon Inkin and CandidaHadi FirmansyahÎncă nu există evaluări
- A Case of Basal Cell Carcinoma Arising in Epidermal Nevus: CameoDocument3 paginiA Case of Basal Cell Carcinoma Arising in Epidermal Nevus: CameoHadi FirmansyahÎncă nu există evaluări
- Lepromatous Leprosy A Case Simulating VerrucousDocument5 paginiLepromatous Leprosy A Case Simulating VerrucousHadi FirmansyahÎncă nu există evaluări
- New Developments in Ochronosis: Review of The LiteratureDocument6 paginiNew Developments in Ochronosis: Review of The LiteratureHadi FirmansyahÎncă nu există evaluări
- Verrucous Lepromatous Leprosy A Rare Form ofDocument4 paginiVerrucous Lepromatous Leprosy A Rare Form ofHadi FirmansyahÎncă nu există evaluări
- Collodion Baby and Loricrin Keratoderma: A Case Report and Mutation AnalysisDocument5 paginiCollodion Baby and Loricrin Keratoderma: A Case Report and Mutation AnalysisHadi FirmansyahÎncă nu există evaluări
- 1999 1 1 29 36Document8 pagini1999 1 1 29 36Hadi FirmansyahÎncă nu există evaluări
- JorgenDocument5 paginiJorgenHadi FirmansyahÎncă nu există evaluări
- DocumentDocument3 paginiDocumentHadi FirmansyahÎncă nu există evaluări
- Cutaneous Annular Sarcoidosis Developing On A Background of Exogenous Ochronosis: A Report of Two Cases and Review of The LiteratureDocument5 paginiCutaneous Annular Sarcoidosis Developing On A Background of Exogenous Ochronosis: A Report of Two Cases and Review of The LiteratureHadi FirmansyahÎncă nu există evaluări
- JorgenDocument5 paginiJorgenHadi FirmansyahÎncă nu există evaluări
- Xerosis CutisDocument6 paginiXerosis CutisHadi FirmansyahÎncă nu există evaluări
- Xerosis CutisDocument6 paginiXerosis CutisHadi FirmansyahÎncă nu există evaluări
- New Developments in Ochronosis: Review of The LiteratureDocument6 paginiNew Developments in Ochronosis: Review of The LiteratureHadi FirmansyahÎncă nu există evaluări
- Patch Test FDEDocument8 paginiPatch Test FDEHadi FirmansyahÎncă nu există evaluări
- Thayer Martin Agar Procedure 08Document1 paginăThayer Martin Agar Procedure 08Hadi FirmansyahÎncă nu există evaluări
- 1486 - Vitamin D PaperDocument9 pagini1486 - Vitamin D PaperHadi FirmansyahÎncă nu există evaluări
- Can P Rio Biotics Prevent VaginitisDocument2 paginiCan P Rio Biotics Prevent VaginitisHadi FirmansyahÎncă nu există evaluări
- Me8072 Renewable Sources of EnergyDocument13 paginiMe8072 Renewable Sources of EnergyNallappan Rajj AÎncă nu există evaluări
- Furuno CA 400Document345 paginiFuruno CA 400Димон100% (3)
- Industrial Internet of Things: Presented To-Presented byDocument18 paginiIndustrial Internet of Things: Presented To-Presented byGaurav RaturiÎncă nu există evaluări
- Digital Signal Processing: B.E Ece (5Th Semester)Document17 paginiDigital Signal Processing: B.E Ece (5Th Semester)Saatwat CoolÎncă nu există evaluări
- Present Simple TaskDocument3 paginiPresent Simple TaskMaria AlejandraÎncă nu există evaluări
- The Variable Resistor Has Been AdjustedDocument3 paginiThe Variable Resistor Has Been AdjustedPank O RamaÎncă nu există evaluări
- 3161 GIS Data ModelsDocument13 pagini3161 GIS Data Modelsapi-3788255Încă nu există evaluări
- Armor MagazineDocument32 paginiArmor Magazine"Rufus"100% (1)
- Efficient Rice Based Cropping SystemDocument24 paginiEfficient Rice Based Cropping Systemsenthilnathan100% (1)
- c083c282a43655ec69532f2704c3993aDocument12 paginic083c282a43655ec69532f2704c3993aAneilRandyRamdialÎncă nu există evaluări
- Inform LetterDocument2 paginiInform LetterMc Suan75% (4)
- A Textual Introduction To Acarya Vasuvan PDFDocument3 paginiA Textual Introduction To Acarya Vasuvan PDFJim LeeÎncă nu există evaluări
- Ii 2015 1Document266 paginiIi 2015 1tuni santeÎncă nu există evaluări
- St. John's Wort: Clinical OverviewDocument14 paginiSt. John's Wort: Clinical OverviewTrismegisteÎncă nu există evaluări
- Manual 35S EnglishDocument41 paginiManual 35S EnglishgugiÎncă nu există evaluări
- Southwest Airlines Final ReportDocument16 paginiSouthwest Airlines Final Reportapi-427311067Încă nu există evaluări
- Tabel Gsi, RMR, RmiDocument4 paginiTabel Gsi, RMR, RmiPup BooÎncă nu există evaluări
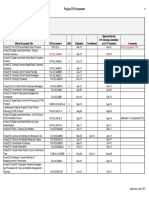
- Approved Project 25 StandardsDocument5 paginiApproved Project 25 StandardsepidavriosÎncă nu există evaluări
- Chapter 04 Product and ServDocument43 paginiChapter 04 Product and ServAlireza AlborziÎncă nu există evaluări