S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Chapter 7: Emotional and Behavioural Problems: DR Jessie EarleDocument28 paginiChapter 7: Emotional and Behavioural Problems: DR Jessie EarlejajmajÎncă nu există evaluări
- 200 Terms & Definition From Pharmacology. WatermarkedDocument17 pagini200 Terms & Definition From Pharmacology. Watermarkedsuresh adgaonkar100% (1)
- OrthopedicDocument1 paginăOrthopedicapi-352507025Încă nu există evaluări
- Can Oral Sex Cause Throat CancerDocument4 paginiCan Oral Sex Cause Throat CancerjyuldipÎncă nu există evaluări
- Emqs ObsDocument33 paginiEmqs Obsbakkiaha100% (1)
- Fascio LaDocument20 paginiFascio LaMuhammad NoorÎncă nu există evaluări
- 6 Metronidazole Drug StudyDocument4 pagini6 Metronidazole Drug Studyshadow gonzalezÎncă nu există evaluări
- Full Text of PT-OT Exam Results (Top 10)Document2 paginiFull Text of PT-OT Exam Results (Top 10)TheSummitExpressÎncă nu există evaluări
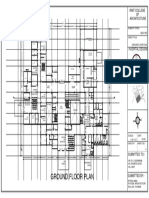
- Ground Floor Plan Sheet 2Document1 paginăGround Floor Plan Sheet 2riteshÎncă nu există evaluări
- SDS - Balloxy HB Light - Comp. B - Marine - Protective - English (Uk) - AustraliaDocument7 paginiSDS - Balloxy HB Light - Comp. B - Marine - Protective - English (Uk) - AustraliaDonÎncă nu există evaluări
- Pediatric Neuropsychology Case Studies PDFDocument358 paginiPediatric Neuropsychology Case Studies PDFGabriela Hernandez100% (1)
- Top 5 Lavender Home RemediesDocument16 paginiTop 5 Lavender Home RemediesjeslynÎncă nu există evaluări
- Police Log November 7, 2016Document13 paginiPolice Log November 7, 2016MansfieldMAPoliceÎncă nu există evaluări
- Medical Surgical Nursing ReviewDocument97 paginiMedical Surgical Nursing ReviewBernadeth Josefa BorelaÎncă nu există evaluări
- Orthofix Investor Presentation - January 2017Document20 paginiOrthofix Investor Presentation - January 2017medtechyÎncă nu există evaluări
- DR Irza Wahid - Annemia Approach - 139Document60 paginiDR Irza Wahid - Annemia Approach - 139single_ladyÎncă nu există evaluări
- Tanggal Rujuk BalnamaDocument7 paginiTanggal Rujuk BalnamapkmjemursariÎncă nu există evaluări
- 1191 Eia en PDFDocument234 pagini1191 Eia en PDFqbich100% (1)
- Asci ReplyDocument5 paginiAsci ReplynupurnluÎncă nu există evaluări
- Traction PDFDocument31 paginiTraction PDFrushaliÎncă nu există evaluări
- JCIA Handbook 2020Document61 paginiJCIA Handbook 2020WAQASÎncă nu există evaluări
- Anti-Protozoal Drugs FinalizedDocument54 paginiAnti-Protozoal Drugs FinalizedMoazama Fayyaz100% (1)
- Mental Health ActDocument48 paginiMental Health ActGursabeen KalraÎncă nu există evaluări
- FCBDocument26 paginiFCBsprapurÎncă nu există evaluări
- Cardiac PoisonsDocument36 paginiCardiac PoisonsTARIQÎncă nu există evaluări
- Paket 2 OkDocument5 paginiPaket 2 OkBerna TodingÎncă nu există evaluări
- Principle of Laser Application in Medicine & LASER SAFETY5Document62 paginiPrinciple of Laser Application in Medicine & LASER SAFETY5melisandrianaÎncă nu există evaluări
- Flip Chart 06 IUDDocument12 paginiFlip Chart 06 IUDLamyaa Ali HasanÎncă nu există evaluări
- Brockton Police Log Updated 10/01/2013Document19 paginiBrockton Police Log Updated 10/01/2013BB0% (1)
- Disease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sDocument84 paginiDisease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sclubstar100% (4)