S-ar putea să vă placă și
- SOP Receiving and Storage of Raw MaterialsDocument2 paginiSOP Receiving and Storage of Raw MaterialsBadethdeth1290% (10)
- Acute Respiratory Distress SyndromeDocument43 paginiAcute Respiratory Distress SyndromeAgnes Pritama Fahmi100% (1)
- Acute Respiratory Distress SyndromeDocument77 paginiAcute Respiratory Distress SyndromeAnnisa Dyah ChairiniÎncă nu există evaluări
- Ventilatorymanagement Ofthenoninjuredlung: David L. Bowton,, Louis Keith ScottDocument10 paginiVentilatorymanagement Ofthenoninjuredlung: David L. Bowton,, Louis Keith ScottGhost11mÎncă nu există evaluări
- Author's Accepted Manuscript: Journal of Cardiothoracic and Vascular AnesthesiaDocument23 paginiAuthor's Accepted Manuscript: Journal of Cardiothoracic and Vascular Anesthesiaricardo villaÎncă nu există evaluări
- 40Document9 pagini40Eduardo SoaresÎncă nu există evaluări
- Ventilation During Lung Resection and Critical Care ComparativeDocument11 paginiVentilation During Lung Resection and Critical Care Comparativeema moralesÎncă nu există evaluări
- Respiratory - ARDS Vent Revised - QuestionsDocument6 paginiRespiratory - ARDS Vent Revised - QuestionsRyan ReÎncă nu există evaluări
- Acuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiesDocument16 paginiAcuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiessamuelÎncă nu există evaluări
- Hfo 2Document9 paginiHfo 2markus_danusantosoÎncă nu există evaluări
- 9mechanical Ventilation in Sepsis-Induced Acute LungDocument6 pagini9mechanical Ventilation in Sepsis-Induced Acute LungTeodora ZamfirescuÎncă nu există evaluări
- Ards 2Document7 paginiArds 2LUCIBELLOT1Încă nu există evaluări
- Ventilation in Acute Lung Injury and ARDS Clinicians' Approaches To MechanicalDocument8 paginiVentilation in Acute Lung Injury and ARDS Clinicians' Approaches To MechanicalEduardo SoaresÎncă nu există evaluări
- Original ResearchDocument8 paginiOriginal ResearchEduardo SoaresÎncă nu există evaluări
- Overventilation and Lung DamageDocument8 paginiOverventilation and Lung DamageDaniel MoralesÎncă nu există evaluări
- The Acute Respiratory Distress Syndrome in 2013: Review Open AccessDocument6 paginiThe Acute Respiratory Distress Syndrome in 2013: Review Open Accessindriyanti natasya ayu utami kottenÎncă nu există evaluări
- Applsci 09 02842 PDFDocument13 paginiApplsci 09 02842 PDFFelicia SutarliÎncă nu există evaluări
- Noninvasive Positive Pressure Ventilation - Successful Outcome in Patients With Acute Lung Injury ARDSDocument6 paginiNoninvasive Positive Pressure Ventilation - Successful Outcome in Patients With Acute Lung Injury ARDSpaulina mancilla ramirezÎncă nu există evaluări
- Newer Modes of Ventilation2Document9 paginiNewer Modes of Ventilation2Saradha PellatiÎncă nu există evaluări
- Kacmarek2020 Article NeurallyAdjustedVentilatoryAssDocument11 paginiKacmarek2020 Article NeurallyAdjustedVentilatoryAssHoracio Panzardo GonzálezÎncă nu există evaluări
- Low-Tidal-Volume Ventilation in The Acute Respiratory Distress SyndromeDocument8 paginiLow-Tidal-Volume Ventilation in The Acute Respiratory Distress SyndromeJimmy Christianto SuryoÎncă nu există evaluări
- VCV Vs PCV in ArdsDocument7 paginiVCV Vs PCV in Ardspaddy9980Încă nu există evaluări
- Terapia Adjunta en SdraDocument23 paginiTerapia Adjunta en SdraMarcoÎncă nu există evaluări
- Effects of Lung Expansion Therapy On Lung Function in Patients With Prolonged Mechanical VentilationDocument7 paginiEffects of Lung Expansion Therapy On Lung Function in Patients With Prolonged Mechanical Ventilationcard breatheÎncă nu există evaluări
- The Acute Respiratory Distress Syndrome: Review SeriesDocument10 paginiThe Acute Respiratory Distress Syndrome: Review Seriesadek07Încă nu există evaluări
- ResuscitationDocument8 paginiResuscitation85tq5nhsqbÎncă nu există evaluări
- Freid 2005Document14 paginiFreid 2005PaulHerreraÎncă nu există evaluări
- Acute Respiratory Distress Syndrome: Clinical ReviewDocument6 paginiAcute Respiratory Distress Syndrome: Clinical ReviewVijeyachandhar DorairajÎncă nu există evaluări
- Ventilación Del Pulmón Sano CC Current 20Document5 paginiVentilación Del Pulmón Sano CC Current 20Silvia Lorena Mireles GonzálezÎncă nu există evaluări
- Acute Respiratory Distress Syndrome Ventilator Management Strategies For AdultsDocument36 paginiAcute Respiratory Distress Syndrome Ventilator Management Strategies For Adultsleokadiobarroso.rjÎncă nu există evaluări
- Complications of Thoracic SurgeryDocument45 paginiComplications of Thoracic SurgeryAlin ToaderÎncă nu există evaluări
- Lung Protective Mechanical Ventilation StrategiesDocument4 paginiLung Protective Mechanical Ventilation StrategiesAnne Julia AgustinÎncă nu există evaluări
- Lung Recruitment Who, When and HowDocument4 paginiLung Recruitment Who, When and HowMahenderaÎncă nu există evaluări
- BMJ Open 2015 ZhangDocument10 paginiBMJ Open 2015 ZhangLuis CordovaÎncă nu există evaluări
- Effect of A Protective-Ventilation Strategy On Mortality in The Acute Respiratory Distress SyndromeDocument8 paginiEffect of A Protective-Ventilation Strategy On Mortality in The Acute Respiratory Distress Syndromeiturraspe12Încă nu există evaluări
- Ajustesiniciales VNIDocument3 paginiAjustesiniciales VNIDamian Torres SperanzaÎncă nu există evaluări
- CcventilacioninicialbuenoDocument3 paginiCcventilacioninicialbuenoARELHI ROSARIO GARCIA MONROYÎncă nu există evaluări
- Acute Respiratory Distress SyndromeDocument6 paginiAcute Respiratory Distress SyndromeNove Mae EscabarteÎncă nu există evaluări
- Mechanical Ventilation - Lessons From The ARDSNet TrialDocument5 paginiMechanical Ventilation - Lessons From The ARDSNet TrialRDG20202Încă nu există evaluări
- Arti Revi 11Document8 paginiArti Revi 11LuLu NikhlaturÎncă nu există evaluări
- 2022-10# (PEERJ) RR in ECMODocument17 pagini2022-10# (PEERJ) RR in ECMOjycntuÎncă nu există evaluări
- VM PediatrikDocument13 paginiVM PediatrikWayan SupiartaÎncă nu există evaluări
- Evid TT 2200305Document4 paginiEvid TT 2200305Muthia Farah AshmaÎncă nu există evaluări
- Original ContributionsDocument9 paginiOriginal ContributionsEduardo SoaresÎncă nu există evaluări
- REVIEW Anesthesia For Thoracic Surgery PDFDocument22 paginiREVIEW Anesthesia For Thoracic Surgery PDFcristinaÎncă nu există evaluări
- Asynchrony Consequences and ManagementDocument17 paginiAsynchrony Consequences and ManagementAna MariaÎncă nu există evaluări
- What Is New in Refractory Hypoxemia 2013Document4 paginiWhat Is New in Refractory Hypoxemia 2013EN BUÎncă nu există evaluări
- Intraoperative Mechanical Ventilation Strategies in Patients Undergoing One-Lung Ventilation: A Meta-AnalysisDocument12 paginiIntraoperative Mechanical Ventilation Strategies in Patients Undergoing One-Lung Ventilation: A Meta-AnalysisdrvmkamathÎncă nu există evaluări
- DefaultDocument37 paginiDefaultBayan Abu AlrubÎncă nu există evaluări
- ArdsDocument69 paginiArdsdrabdallakawareÎncă nu există evaluări
- 28 - Terragni 2012Document7 pagini28 - Terragni 2012Fermin LombardiaÎncă nu există evaluări
- Ventilatorweaningand Extubation: Karen E.A. Burns,, Bram Rochwerg, Andrew J.E. SeelyDocument18 paginiVentilatorweaningand Extubation: Karen E.A. Burns,, Bram Rochwerg, Andrew J.E. Seelyأركان هيلث Arkan healthÎncă nu există evaluări
- Head of Bed ElevationDocument3 paginiHead of Bed ElevationverantikaÎncă nu există evaluări
- Chest: Risk Factors For Extubation Failure in Patients Following A Successful Spontaneous Breathing TrialDocument8 paginiChest: Risk Factors For Extubation Failure in Patients Following A Successful Spontaneous Breathing TrialRodas LisÎncă nu există evaluări
- Rclutamiento VAFO Pre Surfactante PTDocument7 paginiRclutamiento VAFO Pre Surfactante PTGustavo Carhuamaca RoblesÎncă nu există evaluări
- Jurnal Dari Aak 4Document8 paginiJurnal Dari Aak 4rifqi rizalÎncă nu există evaluări
- Chapter 5Document16 paginiChapter 5jess forfodÎncă nu există evaluări
- Acute Respiratory Distress Syndrome, Mechanical Ventilation, and Inhalation Injury in Burn PatientsDocument13 paginiAcute Respiratory Distress Syndrome, Mechanical Ventilation, and Inhalation Injury in Burn Patientspatriciarreis2991Încă nu există evaluări
- Asynchrony Consequences and ManagementDocument17 paginiAsynchrony Consequences and ManagementjuanÎncă nu există evaluări
- Research Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailureDocument7 paginiResearch Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailurewiwiÎncă nu există evaluări
- Essentials in Lung TransplantationDe la EverandEssentials in Lung TransplantationAllan R. GlanvilleÎncă nu există evaluări
- Thesis Prop Trial Print BWDocument18 paginiThesis Prop Trial Print BWOldriana Prawiro HapsariÎncă nu există evaluări
- Precede-Proceed ModelDocument16 paginiPrecede-Proceed ModelOldriana Prawiro Hapsari100% (1)
- Thesis Prop Trial Print BWDocument18 paginiThesis Prop Trial Print BWOldriana Prawiro HapsariÎncă nu există evaluări
- Precede/ProceedDocument10 paginiPrecede/ProceedOldriana Prawiro HapsariÎncă nu există evaluări
- Application of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaDocument10 paginiApplication of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaOldriana Prawiro HapsariÎncă nu există evaluări
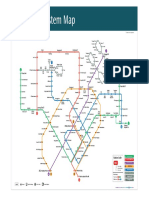
- Singapore Train System MapDocument1 paginăSingapore Train System MapOldriana Prawiro HapsariÎncă nu există evaluări
- Ad and Ar InheritanceDocument45 paginiAd and Ar InheritanceOldriana Prawiro HapsariÎncă nu există evaluări
- Thyroid Disease in PregnancyDocument12 paginiThyroid Disease in PregnancyOldriana Prawiro HapsariÎncă nu există evaluări
- O IntegratedscienceDocument36 paginiO IntegratedscienceFarai FaustosÎncă nu există evaluări
- Group Activity 1 - BAFF MatrixDocument1 paginăGroup Activity 1 - BAFF MatrixGreechiane LongoriaÎncă nu există evaluări
- School Form 2 (SF2) Daily Attendance Report of LearnersDocument4 paginiSchool Form 2 (SF2) Daily Attendance Report of LearnersRyan A. CabalidaÎncă nu există evaluări
- Toolbox Talk 9: Critical Risks - ExcavationsDocument2 paginiToolbox Talk 9: Critical Risks - ExcavationsPravin GowardunÎncă nu există evaluări
- Case Write Up 3Document4 paginiCase Write Up 3E learningÎncă nu există evaluări
- Planning PlaygroundDocument16 paginiPlanning PlaygroundAdnan AliÎncă nu există evaluări
- Regulatory Compliance Planning GuideDocument70 paginiRegulatory Compliance Planning GuideriestgÎncă nu există evaluări
- Talent MappingDocument18 paginiTalent MappingSoumya RanjanÎncă nu există evaluări
- Pulpal DiseasesDocument34 paginiPulpal Diseasessamar yousif mohamedÎncă nu există evaluări
- India's #1 Nroute Daily Whey Protein Powder Online 2022Document3 paginiIndia's #1 Nroute Daily Whey Protein Powder Online 2022NRoute ProteinÎncă nu există evaluări
- HârnWorld - Fyvria (CG 4505)Document36 paginiHârnWorld - Fyvria (CG 4505)Vlad T100% (1)
- A Beauty 671-680Document29 paginiA Beauty 671-680YollyÎncă nu există evaluări
- Fun Games - 1 Min Game 01Document9 paginiFun Games - 1 Min Game 01Purvi ShahÎncă nu există evaluări
- TinnitusDocument34 paginiTinnitusHnia UsmanÎncă nu există evaluări
- Abs & Core Workout Calendar - Mar 2020Document1 paginăAbs & Core Workout Calendar - Mar 2020Claudia anahiÎncă nu există evaluări
- Araldite - GT7074Document2 paginiAraldite - GT7074maz234Încă nu există evaluări
- A Theory of The Human Need For OccupationDocument9 paginiA Theory of The Human Need For OccupationNel HinilzaÎncă nu există evaluări
- Tsoukaki 2012Document8 paginiTsoukaki 2012Marina JoelÎncă nu există evaluări
- 16-Week Harvey Walden MarathonTraining PlanDocument18 pagini16-Week Harvey Walden MarathonTraining PlanKaren MiranoÎncă nu există evaluări
- The WTO and Developing Countries: The Missing: Link of International Distributive JusticeDocument395 paginiThe WTO and Developing Countries: The Missing: Link of International Distributive JusticeMuhammad SajidÎncă nu există evaluări
- Hazops Should Be Fun - The Stream-Based HazopDocument77 paginiHazops Should Be Fun - The Stream-Based HazopHector Tejeda100% (1)
- Sample Paper 1Document36 paginiSample Paper 1Annshai Jam MetanteÎncă nu există evaluări
- Satvik DietDocument3 paginiSatvik DietDisha TÎncă nu există evaluări
- Selenia Ultra 45 EOL Letter v4Document1 paginăSelenia Ultra 45 EOL Letter v4srinibmeÎncă nu există evaluări
- Antitrombotik, PPT 7Document66 paginiAntitrombotik, PPT 7Rizky Saraswati IndraputriÎncă nu există evaluări
- Interview Marsha SarverDocument3 paginiInterview Marsha Sarverapi-326930615Încă nu există evaluări
- The CSI Effect - Google FormsDocument12 paginiThe CSI Effect - Google FormsZivi DegenÎncă nu există evaluări
- 1 s2.0 S2667368123000116 MainDocument24 pagini1 s2.0 S2667368123000116 MainCelia MartinezÎncă nu există evaluări
- Office: The of The SecretaryDocument20 paginiOffice: The of The SecretaryJustine KimÎncă nu există evaluări