S-ar putea să vă placă și
- DelacruzDocument10 paginiDelacruzapi-510887381Încă nu există evaluări
- Effect of Chest PackDocument2 paginiEffect of Chest PacksureshbabubnysÎncă nu există evaluări
- What Is Autism? by James Jeffrey Bradstreet, MD, MD (H), FAAFPDocument4 paginiWhat Is Autism? by James Jeffrey Bradstreet, MD, MD (H), FAAFPautismoneÎncă nu există evaluări
- Admissions On Every Friday: Correspondence Address Campus AddressDocument6 paginiAdmissions On Every Friday: Correspondence Address Campus Addresshitesh_tilalaÎncă nu există evaluări
- UB Naturopathy's: Science-Ejected Vitalism, Autoentheism & Such WooDocument3 paginiUB Naturopathy's: Science-Ejected Vitalism, Autoentheism & Such WoodaijiyobuÎncă nu există evaluări
- CNW - Nov13-2007 - Health Canada Approves Health Claim For HMS 90 - ImmunocalDocument1 paginăCNW - Nov13-2007 - Health Canada Approves Health Claim For HMS 90 - Immunocalapi-3714923Încă nu există evaluări
- BioenergyGlovesManual 2Document33 paginiBioenergyGlovesManual 2Irina Liana DimaÎncă nu există evaluări
- HomeopathyArcCourse DetailDocument11 paginiHomeopathyArcCourse DetailRajiv SharmaÎncă nu există evaluări
- Importance of Yog in NaturopathyDocument3 paginiImportance of Yog in NaturopathyAbhaya Raj UpadhayaÎncă nu există evaluări
- Autismul DPDV GeneticDocument10 paginiAutismul DPDV GeneticnkhskquiÎncă nu există evaluări
- Piyas Utsav ProgramDocument4 paginiPiyas Utsav ProgramdrmbalarÎncă nu există evaluări
- Homeopathy in ColombiaDocument23 paginiHomeopathy in ColombiaFelipe CárdenasÎncă nu există evaluări
- NaturopathyDocument3 paginiNaturopathyWalter TripÎncă nu există evaluări
- Recovering Mark by Cynthia Macluskie and Mark Makes A Difference! by Mark MacluskieDocument2 paginiRecovering Mark by Cynthia Macluskie and Mark Makes A Difference! by Mark MacluskieautismoneÎncă nu există evaluări
- Sexual Recovery Institute - Summer & Fall Saturday Lecture SeriesDocument2 paginiSexual Recovery Institute - Summer & Fall Saturday Lecture SeriesSexRecoveryÎncă nu există evaluări
- Understanding and Taming Hyperacidity: An AYUSH PerspectiveDocument3 paginiUnderstanding and Taming Hyperacidity: An AYUSH PerspectiveHomoeopathic PulseÎncă nu există evaluări
- Cutler Counting RulesDocument2 paginiCutler Counting RulesRobertÎncă nu există evaluări
- Diabetes Without Needles: Non-invasive Diagnostics and Health ManagementDe la EverandDiabetes Without Needles: Non-invasive Diagnostics and Health ManagementÎncă nu există evaluări
- Naturopathy and Yogic Question Papers Free Downloads - B.nat - University of Madras PDFDocument4 paginiNaturopathy and Yogic Question Papers Free Downloads - B.nat - University of Madras PDFমুখোমুখিহৃদয়Încă nu există evaluări
- West Nile Virus Homeopathy HandoutDocument3 paginiWest Nile Virus Homeopathy HandoutRoger Auge100% (1)
- New Post Grad ProgramDocument8 paginiNew Post Grad ProgramPradeep KumarÎncă nu există evaluări
- HomeopathyDocument11 paginiHomeopathyGurudutt BannikodÎncă nu există evaluări
- Methylcobalamin (MB12) Nasal Spray Summary - by Stan Kurtz - Autism, ADHD, Asthma, Eczema, and Chronic Fatigue RecoveryDocument5 paginiMethylcobalamin (MB12) Nasal Spray Summary - by Stan Kurtz - Autism, ADHD, Asthma, Eczema, and Chronic Fatigue RecoveryRoberto ScafidiÎncă nu există evaluări
- Predictive Homeopathy IIDocument4 paginiPredictive Homeopathy IIantoscriÎncă nu există evaluări
- NaturopathyDocument2 paginiNaturopathyyhettÎncă nu există evaluări
- State of West Virginia Ex Rel. Recep : Honorable: - I-P-294 JudgeDocument21 paginiState of West Virginia Ex Rel. Recep : Honorable: - I-P-294 JudgeAnna SaundersÎncă nu există evaluări
- Autism Spectrum Disorders BlogDocument3 paginiAutism Spectrum Disorders BlogspeechendeavorsÎncă nu există evaluări
- AutismAdvisoryPanelReport 2019Document64 paginiAutismAdvisoryPanelReport 2019CityNewsTorontoÎncă nu există evaluări
- Naturopathic Medicine: A Short HistoryDocument3 paginiNaturopathic Medicine: A Short HistoryRoseanne Legaspi CasayuranÎncă nu există evaluări
- Finding Mary: One Family’S Journey on the Road to Autism RecoveryDe la EverandFinding Mary: One Family’S Journey on the Road to Autism RecoveryÎncă nu există evaluări
- Autism AmishDocument2 paginiAutism AmishPower one100% (1)
- Predictive HomeopathyDocument5 paginiPredictive HomeopathyantoscriÎncă nu există evaluări
- Whole Group Lesson Plan RevisedDocument6 paginiWhole Group Lesson Plan Revisedapi-458954188Încă nu există evaluări
- Autism IUQuestions and Advanced-CLDocument10 paginiAutism IUQuestions and Advanced-CLMd Jakir HossainÎncă nu există evaluări
- Healing & Curing Center (Natural Way)Document30 paginiHealing & Curing Center (Natural Way)amurutha saiÎncă nu există evaluări
- Carly Voice Breaking Through Autism 470467 PDFDocument6 paginiCarly Voice Breaking Through Autism 470467 PDFFederico DcfÎncă nu există evaluări
- Organon EssayDocument9 paginiOrganon EssayNicola CrevisÎncă nu există evaluări
- Acrodynia ASD in Survivor's FamiliesANCESTRY OF PINK DISEASE (INFANTILE ACRODYNIA) IDENTIFIED AS A RISK FACTOR FOR AUTISM SPECTRUM DISORDERSDocument10 paginiAcrodynia ASD in Survivor's FamiliesANCESTRY OF PINK DISEASE (INFANTILE ACRODYNIA) IDENTIFIED AS A RISK FACTOR FOR AUTISM SPECTRUM DISORDERS23980hcasdjknÎncă nu există evaluări
- AuyrvedaDocument22 paginiAuyrvedaapi-288733554Încă nu există evaluări
- Living and Working With Children With Autism Spectrum DisorderDocument70 paginiLiving and Working With Children With Autism Spectrum DisorderShams JhugrooÎncă nu există evaluări
- HomeopathyDocument16 paginiHomeopathygregotza0% (1)
- Rada, R. E. Controversial Issues in Treating The Dental Patient With Autism.Document7 paginiRada, R. E. Controversial Issues in Treating The Dental Patient With Autism.hollyÎncă nu există evaluări
- HomeopathyDocument18 paginiHomeopathysai prem0% (1)
- Nosodes Sarcodes HomeopathyDocument35 paginiNosodes Sarcodes HomeopathydrdivishÎncă nu există evaluări
- Caroline - Walrad - The Autistic Spectrum NotesDocument14 paginiCaroline - Walrad - The Autistic Spectrum Notesnamkay_tenzynÎncă nu există evaluări
- Yoga Ans NaturopathyDocument10 paginiYoga Ans NaturopathyMichele PóÎncă nu există evaluări
- Living With AutismDocument115 paginiLiving With Autismjjrelucio3748Încă nu există evaluări
- Case Study - Seizuring DogDocument8 paginiCase Study - Seizuring Dogapi-301746262Încă nu există evaluări
- Visuals of HomeopathyDocument8 paginiVisuals of HomeopathyDubi RonenÎncă nu există evaluări
- SafeMinds, Wanted To Be at The Hearing But Couldn't.Document29 paginiSafeMinds, Wanted To Be at The Hearing But Couldn't.Heather X RhodesÎncă nu există evaluări
- Katelyn Wright Capstone Unit 5 Naturopathy Lecture NotesDocument11 paginiKatelyn Wright Capstone Unit 5 Naturopathy Lecture Notesapi-541137348Încă nu există evaluări
- ESSAY - Homoeopathy Vs AllopathyDocument4 paginiESSAY - Homoeopathy Vs AllopathyAbhishek TomarÎncă nu există evaluări
- Yurveda and Naturopathy CentersDocument4 paginiYurveda and Naturopathy CentersPriya MakwanaÎncă nu există evaluări
- Computer Aided Learning in OrganonDocument36 paginiComputer Aided Learning in OrganonSaurav AroraÎncă nu există evaluări
- Best Autism Treatment in ChennaiDocument32 paginiBest Autism Treatment in ChennaiNP KarthikeyenÎncă nu există evaluări
- Drug De-AddictionDocument19 paginiDrug De-AddictionClaudia De Rosa0% (1)
- Photobiology PPT by DR AkbarDocument27 paginiPhotobiology PPT by DR AkbarAyesha awanÎncă nu există evaluări
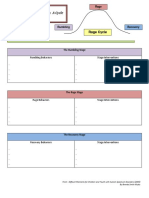
- Rumbling Rage Recovery InfographicDocument4 paginiRumbling Rage Recovery Infographicapi-247044545Încă nu există evaluări
- Test - Unit 1: Online Sales Course in Strategic Sales ManagementDocument7 paginiTest - Unit 1: Online Sales Course in Strategic Sales ManagementankitÎncă nu există evaluări
- Member Check ListDocument4 paginiMember Check ListankitÎncă nu există evaluări
- Pre-Assessment Guidelines and Forms: Nabh-Ayush-PaDocument10 paginiPre-Assessment Guidelines and Forms: Nabh-Ayush-PaankitÎncă nu există evaluări
- Policy & Guideline For Use of TrademarkDocument8 paginiPolicy & Guideline For Use of TrademarkankitÎncă nu există evaluări
- General Information On NABHDocument18 paginiGeneral Information On NABHankitÎncă nu există evaluări
- Agreement Approved NewDocument12 paginiAgreement Approved NewVishnu Teja ReddyÎncă nu există evaluări
- Wellness Profile FICCIDocument5 paginiWellness Profile FICCIkarthikponnapaÎncă nu există evaluări
- (WWW - Entrance-Exam - Net) - List of It Companies in Ahmedabad and GandhinagarDocument8 pagini(WWW - Entrance-Exam - Net) - List of It Companies in Ahmedabad and GandhinagarankitÎncă nu există evaluări
- List of Books - GodeliteDocument1 paginăList of Books - GodeliteankitÎncă nu există evaluări
- Agency AgreementDocument27 paginiAgency AgreementankitÎncă nu există evaluări
- Respondent t10Document19 paginiRespondent t10shreeyasingh0929Încă nu există evaluări
- Mercury Toxicity and Systemic Elimination Agents Mercola KlinghartDocument10 paginiMercury Toxicity and Systemic Elimination Agents Mercola KlinghartzaskribdoÎncă nu există evaluări
- Verhaeghen Borchelt Smith 2003Document11 paginiVerhaeghen Borchelt Smith 2003paulverhaeghen6877Încă nu există evaluări
- Behavioral Pain Scale (BPS) For Pain Assessment in Intubated Patients - MDCalcDocument2 paginiBehavioral Pain Scale (BPS) For Pain Assessment in Intubated Patients - MDCalcJeane SuyantoÎncă nu există evaluări
- MidazolamDocument2 paginiMidazolamDesireemae Riosa-Candaroma100% (6)
- ICD-11 An International Classification of DiseasesDocument11 paginiICD-11 An International Classification of DiseasesVictoria HavrylivÎncă nu există evaluări
- CPG Management of Hypertension (4th Edition)Document98 paginiCPG Management of Hypertension (4th Edition)ssfdsÎncă nu există evaluări
- NCP AnxietyDocument1 paginăNCP AnxietyUnang MagnayeÎncă nu există evaluări
- Entrevista BjornDocument11 paginiEntrevista BjornMirza GlusacÎncă nu există evaluări
- 2.PMS Report Template GRF - 25-46a - Rev - 1.2 - PMS - Appplication - FormDocument8 pagini2.PMS Report Template GRF - 25-46a - Rev - 1.2 - PMS - Appplication - Formdelal karakuÎncă nu există evaluări
- Textbook of Pleural Diseases (2008)Document673 paginiTextbook of Pleural Diseases (2008)Alexandra NicaÎncă nu există evaluări
- Generic MedicinesDocument16 paginiGeneric MedicinesAnn Christine C. ChuaÎncă nu există evaluări
- Nimotuzumab A Novel anti-EGFR Monoclonal PDFDocument8 paginiNimotuzumab A Novel anti-EGFR Monoclonal PDFAkbar SuuryoÎncă nu există evaluări
- BurnDocument3 paginiBurnhameunjungÎncă nu există evaluări
- The Patient Was Taken To The Emergency RoomDocument2 paginiThe Patient Was Taken To The Emergency RoomAndika Ridho MÎncă nu există evaluări
- Sop For Public HealthDocument1 paginăSop For Public HealthAyomiposi OloniniyiÎncă nu există evaluări
- AIA HealthShield Gold MaxDocument16 paginiAIA HealthShield Gold Maxmailer686Încă nu există evaluări
- Larynx, Trachea, Lung and PleuraDocument60 paginiLarynx, Trachea, Lung and PleuraKatÎncă nu există evaluări
- Pendidikan Pasien Cath LabDocument10 paginiPendidikan Pasien Cath LabAgnesthesiaÎncă nu există evaluări
- CCRT WitzekDocument15 paginiCCRT WitzekMario Antonio FloresÎncă nu există evaluări
- p2 Exam ReviewerDocument20 paginip2 Exam ReviewerChristopher Andrei Salonga LimÎncă nu există evaluări
- Pulmonology Techniques Breakthrough by Slidesgo 2Document33 paginiPulmonology Techniques Breakthrough by Slidesgo 2BEATRIZ MACEDO VALADÃOÎncă nu există evaluări
- Syndrome Differentiation According To The Eight Principles - TCM Basic Principles ShennongDocument5 paginiSyndrome Differentiation According To The Eight Principles - TCM Basic Principles ShennongYi-Ying LuÎncă nu există evaluări
- Basic Ercp InterpretationDocument19 paginiBasic Ercp Interpretationhoneyworks100% (2)
- Signature Seminar Series MyopiaDocument1 paginăSignature Seminar Series MyopiaNiero GalangÎncă nu există evaluări
- Funding Agencies Links 1 1Document3 paginiFunding Agencies Links 1 1RishavÎncă nu există evaluări
- Raynaud'S Phenomenon: Dr. Ajay Panwar Japi (May 2010)Document23 paginiRaynaud'S Phenomenon: Dr. Ajay Panwar Japi (May 2010)Ajay PanwarÎncă nu există evaluări
- NCM 102 Care of Mother, Child, and Population Group at Risk or With ProblemsDocument33 paginiNCM 102 Care of Mother, Child, and Population Group at Risk or With ProblemsAyman DaudÎncă nu există evaluări
- ThesisDocument197 paginiThesisAnil BatraÎncă nu există evaluări
- Chagrin Factor - Feinstein1985Document3 paginiChagrin Factor - Feinstein1985Rafael MartinsÎncă nu există evaluări