S-ar putea să vă placă și
- S HPVDocument3 paginiS HPVAnibal Rodríguez MerinoÎncă nu există evaluări
- Salud PublicaDocument24 paginiSalud PublicaPR3M1UMÎncă nu există evaluări
- SALUD PÚBLICA 20 Mayo 2015 OficialDocument37 paginiSALUD PÚBLICA 20 Mayo 2015 OficialPR3M1UMÎncă nu există evaluări
- Investigacion de Brotes CEAL Honduras 2007 Definitiva 1Document24 paginiInvestigacion de Brotes CEAL Honduras 2007 Definitiva 1PR3M1UMÎncă nu există evaluări
- Consenso VPH 2002Document57 paginiConsenso VPH 2002Maria Alejandra Quispe FloresÎncă nu există evaluări
- Comunicacion 1U-5Document61 paginiComunicacion 1U-5PR3M1UMÎncă nu există evaluări
- Hemograma CompletoDocument2 paginiHemograma CompletoFernando RamirezÎncă nu există evaluări
- Seimc Procedimientomicrobiologia1aDocument27 paginiSeimc Procedimientomicrobiologia1aRobert MendietaÎncă nu există evaluări
- Control de La CalidadDocument46 paginiControl de La CalidadClaudia Leticia Mendoza MacíasÎncă nu există evaluări
- APUNTE Micosis y Diangostico MicologicoDocument16 paginiAPUNTE Micosis y Diangostico MicologicoVero RodrgÎncă nu există evaluări
- Resistencia en Cocos Gram PositivosDocument13 paginiResistencia en Cocos Gram PositivosPR3M1UMÎncă nu există evaluări
- Enterococos PDFDocument15 paginiEnterococos PDFPR3M1UMÎncă nu există evaluări
- Ictericia NeonatalDocument18 paginiIctericia Neonataljose_luis_408Încă nu există evaluări
- Manual de CosDocument248 paginiManual de CosfcalarconÎncă nu există evaluări
- INMUNOENSAYOSDocument150 paginiINMUNOENSAYOSquimico clinico 27100% (16)
- P7 E202 S132 A2258Document6 paginiP7 E202 S132 A2258PR3M1UMÎncă nu există evaluări
- CististisDocument4 paginiCististisLacho68Încă nu există evaluări
- Hematuria y Proteinuria en DeporteDocument57 paginiHematuria y Proteinuria en DeporteleslesÎncă nu există evaluări
- Micro HematuriaDocument7 paginiMicro HematuriaPR3M1UMÎncă nu există evaluări
- Micro HematuriaDocument7 paginiMicro HematuriaPR3M1UMÎncă nu există evaluări
- Mas Allá Del ABO 2 PDFDocument47 paginiMas Allá Del ABO 2 PDFPR3M1UM100% (1)
- AESM. Calidad en El Laboratorio de Bioquimica-Concepto, Herramientas y Ejemplos de AplicacionDocument23 paginiAESM. Calidad en El Laboratorio de Bioquimica-Concepto, Herramientas y Ejemplos de Aplicacioncolve87Încă nu există evaluări
- Unidad 1 ParasitologiaDocument10 paginiUnidad 1 ParasitologiajuanetitoÎncă nu există evaluări
- Manual de Mantenimiento para Equipos de LaboratorioDocument212 paginiManual de Mantenimiento para Equipos de LaboratorioMiguel Angel100% (6)
- Programa de Salud y Seguridad en El Area de Trabajo 2103-07-23Document47 paginiPrograma de Salud y Seguridad en El Area de Trabajo 2103-07-23PR3M1UMÎncă nu există evaluări
- Manual Bioseguridad ISPCHDocument46 paginiManual Bioseguridad ISPCHJoão José Damian Salazar100% (1)
- Examengeneraldeorina 110312090829 Phpapp01Document91 paginiExamengeneraldeorina 110312090829 Phpapp01PR3M1UMÎncă nu există evaluări
- Programa de Salud y Seguridad en El Area de Trabajo 2103-07-23Document47 paginiPrograma de Salud y Seguridad en El Area de Trabajo 2103-07-23PR3M1UMÎncă nu există evaluări
- GLOMERULOPATIASDocument124 paginiGLOMERULOPATIASGianella Peña MendozaÎncă nu există evaluări
- Diagnostico Del Sindrome de CushingDocument8 paginiDiagnostico Del Sindrome de CushingPriscila Ron LoaizaÎncă nu există evaluări
- ETMR5 ComDocument88 paginiETMR5 ComrollnnyÎncă nu există evaluări
- Criterios PatologiaDocument88 paginiCriterios PatologiaCamille KirschbaumÎncă nu există evaluări
- Apuntes OncologíaDocument353 paginiApuntes OncologíaDiego Pedraza GarciaÎncă nu există evaluări
- Seminario 1Document6 paginiSeminario 1titanusÎncă nu există evaluări
- 5 Leyes Biologicas Dr. Hamer. PublicacionDocument36 pagini5 Leyes Biologicas Dr. Hamer. Publicaciondrago100% (1)
- Nod 32 2019Document10 paginiNod 32 2019alvaro.alvaroÎncă nu există evaluări
- Suplemento Mineral ReforzadoDocument15 paginiSuplemento Mineral ReforzadoCarlos Alberto Gibaja ZapataÎncă nu există evaluări
- Triptico Cruz RojaDocument2 paginiTriptico Cruz RojaJoselyn Tamara Rivera RojasÎncă nu există evaluări
- Prueba de Desarrollo Tildación-2Document6 paginiPrueba de Desarrollo Tildación-2mercedesÎncă nu există evaluări
- Plan Regional de CancerDocument20 paginiPlan Regional de CancerObstetra Ydelsa DelgadoÎncă nu există evaluări
- Cancer de Mama ChingonDocument3 paginiCancer de Mama ChingonRebeca VazquezÎncă nu există evaluări
- Endocrinología: Metabolismo Del Calcio y FósforoDocument10 paginiEndocrinología: Metabolismo Del Calcio y FósforoMireya Cuevas SosaÎncă nu există evaluări
- Ay Laviu MadreDocument28 paginiAy Laviu MadreDaniel RosalesÎncă nu există evaluări
- 45 Formas para Quemar Calorías FácilmenteDocument38 pagini45 Formas para Quemar Calorías FácilmenteEduardoÎncă nu există evaluări
- Cuidados en El PuerperioDocument6 paginiCuidados en El PuerperioVict SanÎncă nu există evaluări
- Cirugía MamariaDocument10 paginiCirugía MamariaGisela AlvarezÎncă nu există evaluări
- Introduccion A La Clinica Med 3100Document4 paginiIntroduccion A La Clinica Med 3100Heidy Lisbeth Medina100% (1)
- Diabetes Noticias BoliviaDocument3 paginiDiabetes Noticias BoliviaJesúsQuispeCopaÎncă nu există evaluări
- Neutropenia Febril. Concenso SAPDocument26 paginiNeutropenia Febril. Concenso SAPVelen PenniniÎncă nu există evaluări
- Diapositivas Del Sistema DigestivoDocument19 paginiDiapositivas Del Sistema DigestivoVivian Arrieta Silva100% (3)
- Cáncer Biliar Pancreático y EncrucijadaDocument2 paginiCáncer Biliar Pancreático y EncrucijadagdfdgÎncă nu există evaluări
- Cirrosis HepáticaDocument23 paginiCirrosis HepáticaEmilyDavilaSotoÎncă nu există evaluări
- Onco - GastroDocument9 paginiOnco - GastroCarolina RuizÎncă nu există evaluări
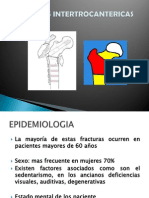
- Fracturas IntertrocantericasDocument38 paginiFracturas IntertrocantericasCarolina SalgueroÎncă nu există evaluări
- GMM - Vol - 149 - 1 - 2013 ARTÍCULODocument129 paginiGMM - Vol - 149 - 1 - 2013 ARTÍCULOMANISSABELLA0% (1)
- Caso Clínico Accidente LaboralDocument12 paginiCaso Clínico Accidente LaboraldianaÎncă nu există evaluări
- Rayos X PolitraumatismoDocument7 paginiRayos X PolitraumatismobrigetteÎncă nu există evaluări
- Recupera tu mente, reconquista tu vidaDe la EverandRecupera tu mente, reconquista tu vidaEvaluare: 5 din 5 stele5/5 (6)
- El Monje Que Vendio Su Ferrari: Una Fábula EspiritualDe la EverandEl Monje Que Vendio Su Ferrari: Una Fábula EspiritualEvaluare: 4.5 din 5 stele4.5/5 (1698)
- Tus Zonas Erroneas: Guía Para Combatir las Causas de la InfelicidadDe la EverandTus Zonas Erroneas: Guía Para Combatir las Causas de la InfelicidadEvaluare: 4.5 din 5 stele4.5/5 (1831)
- Psicología oscura: Una guía esencial de persuasión, manipulación, engaño, control mental, negociación, conducta humana, PNL y guerra psicológicaDe la EverandPsicología oscura: Una guía esencial de persuasión, manipulación, engaño, control mental, negociación, conducta humana, PNL y guerra psicológicaEvaluare: 4.5 din 5 stele4.5/5 (766)
- Tu cerebro emocional: Saca partido de lo que sientes y transforma tu vidaDe la EverandTu cerebro emocional: Saca partido de lo que sientes y transforma tu vidaEvaluare: 5 din 5 stele5/5 (2)
- Cómo hacer que te pasen cosas buenas: Entiende tu cerebro, gestiona tus emociones, mejora tu vidaDe la EverandCómo hacer que te pasen cosas buenas: Entiende tu cerebro, gestiona tus emociones, mejora tu vidaEvaluare: 5 din 5 stele5/5 (1870)
- La revolución de la glucosa: Equilibra tus niveles de glucosa y cambiarás tu salud y tu vidaDe la EverandLa revolución de la glucosa: Equilibra tus niveles de glucosa y cambiarás tu salud y tu vidaEvaluare: 5 din 5 stele5/5 (201)
- Yo Pude, ¡Tú Puedes!: Cómo tomar el control de tu bienestar emocional y convertirte en una persona imparable (edición revisada y expandida)De la EverandYo Pude, ¡Tú Puedes!: Cómo tomar el control de tu bienestar emocional y convertirte en una persona imparable (edición revisada y expandida)Evaluare: 5 din 5 stele5/5 (7)
- Cómo Acertar en tu Nueva Relación de Pareja: Todas las claves para saber si tu relación tiene futuro... o te conviene salir corriendo de ahí.De la EverandCómo Acertar en tu Nueva Relación de Pareja: Todas las claves para saber si tu relación tiene futuro... o te conviene salir corriendo de ahí.Evaluare: 4.5 din 5 stele4.5/5 (7)
- Resetea tu mente. Descubre de lo que eres capazDe la EverandResetea tu mente. Descubre de lo que eres capazEvaluare: 5 din 5 stele5/5 (196)
- Los Secretos De La Mente Millonaria: Domina el juego de la riquezaDe la EverandLos Secretos De La Mente Millonaria: Domina el juego de la riquezaEvaluare: 5 din 5 stele5/5 (457)
- ¡Tómate un respiro! Mindfulness: El arte de mantener la calma en medio de la tempestadDe la Everand¡Tómate un respiro! Mindfulness: El arte de mantener la calma en medio de la tempestadEvaluare: 5 din 5 stele5/5 (198)
- ¿Por qué mis padres no me aman?: Empezando a sanarDe la Everand¿Por qué mis padres no me aman?: Empezando a sanarEvaluare: 4.5 din 5 stele4.5/5 (33)
- Resumen de Pensar rápido pensar despacio de Daniel KahnemanDe la EverandResumen de Pensar rápido pensar despacio de Daniel KahnemanEvaluare: 4.5 din 5 stele4.5/5 (64)
- Homo antecessor: El nacimiento de una especieDe la EverandHomo antecessor: El nacimiento de una especieEvaluare: 5 din 5 stele5/5 (1)
- Mindfulness para principiantes: Medita sin meditarDe la EverandMindfulness para principiantes: Medita sin meditarEvaluare: 5 din 5 stele5/5 (53)
- Disciplina Mental: Técnicas infalibles para lograr todo lo que te propones y eliminar la pereza y la procrastinación de tu vida para siempreDe la EverandDisciplina Mental: Técnicas infalibles para lograr todo lo que te propones y eliminar la pereza y la procrastinación de tu vida para siempreEvaluare: 5 din 5 stele5/5 (3)
- El poder del optimismo: Herramientas para vivir de forma más positivaDe la EverandEl poder del optimismo: Herramientas para vivir de forma más positivaEvaluare: 5 din 5 stele5/5 (16)
- Influencia. La psicología de la persuasiónDe la EverandInfluencia. La psicología de la persuasiónEvaluare: 4.5 din 5 stele4.5/5 (14)
- Grimorio: Cómo lanzar y elaborar hechizos mágicos, aprender las prácticas wiccanas y desvelar los secretos de la brujería a través de un diario ritualDe la EverandGrimorio: Cómo lanzar y elaborar hechizos mágicos, aprender las prácticas wiccanas y desvelar los secretos de la brujería a través de un diario ritualÎncă nu există evaluări
- Zensorialmente : Dejá que tu cuerpo sea tu cerebroDe la EverandZensorialmente : Dejá que tu cuerpo sea tu cerebroÎncă nu există evaluări