S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Emailing CPG-E PDFDocument206 paginiEmailing CPG-E PDFCarlos H. AcuñaÎncă nu există evaluări
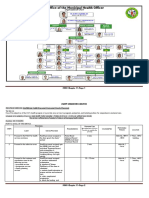
- Municipal Health Organizational ChartDocument10 paginiMunicipal Health Organizational ChartJPJessiePaulÎncă nu există evaluări
- PCCP CAP Guidelines 2016 Update PDFDocument23 paginiPCCP CAP Guidelines 2016 Update PDFFarr Krizha TangkusanÎncă nu există evaluări
- Phil National Drug Formulary Vol1ed7 - 2008Document315 paginiPhil National Drug Formulary Vol1ed7 - 2008Diego A. Veloso III100% (5)
- DOH Annual Report 2015Document28 paginiDOH Annual Report 2015Jade MonrealÎncă nu există evaluări
- Phil National Drug Formulary Vol1ed7 - 2008Document315 paginiPhil National Drug Formulary Vol1ed7 - 2008Diego A. Veloso III100% (5)
- Respiratory PhysiologyDocument10 paginiRespiratory PhysiologyJPJessiePaul100% (1)
- Survey Tool Dummy TableDocument10 paginiSurvey Tool Dummy TableJPJessiePaulÎncă nu există evaluări
- DOH Revised Clinical Guidelines - DENGUE PDFDocument27 paginiDOH Revised Clinical Guidelines - DENGUE PDFRey San Luis III0% (1)
- E BM White PaperDocument14 paginiE BM White PaperpongidaeÎncă nu există evaluări
- InControl Publication Fatigue in CKDDocument8 paginiInControl Publication Fatigue in CKDJPJessiePaulÎncă nu există evaluări
- AHA Beneficial Effects of Afterload Reducing Agents in Patients With CHF and Aortic StenosisDocument6 paginiAHA Beneficial Effects of Afterload Reducing Agents in Patients With CHF and Aortic StenosisJPJessiePaulÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Dermawound Original Venous Stasis Wound CareDocument8 paginiDermawound Original Venous Stasis Wound CareNew Medical Solutions - Your Source for Dermawound, BurnBGone and more...Încă nu există evaluări
- Pa Australian Guidelines On Adhd Draft PDFDocument291 paginiPa Australian Guidelines On Adhd Draft PDFJonÎncă nu există evaluări
- 2015 Nature Glypican 1 Identifies Cancer ExosomesDocument24 pagini2015 Nature Glypican 1 Identifies Cancer ExosomesAgata HugglerÎncă nu există evaluări
- Respiratory Acidosis: Dr. Ann Valerie F. Habana Critical Care MedicineDocument21 paginiRespiratory Acidosis: Dr. Ann Valerie F. Habana Critical Care Medicineannv748687Încă nu există evaluări
- ETS & CapillaryDocument6 paginiETS & CapillaryRoela Marie AlbaniaÎncă nu există evaluări
- Ardc 2Document1 paginăArdc 2Camille GuintoÎncă nu există evaluări
- CHN SummaryDocument20 paginiCHN SummaryFaith ManingoÎncă nu există evaluări
- A Cross-Cultural Exploratory Analysis of Pandemic Growth - The Case of Covid 19Document22 paginiA Cross-Cultural Exploratory Analysis of Pandemic Growth - The Case of Covid 19gabriel6birsan-1Încă nu există evaluări
- I 693instrDocument11 paginiI 693instrShivana SeeramÎncă nu există evaluări
- 001 Diagnosis of Neurological DiseaseDocument7 pagini001 Diagnosis of Neurological DiseasemgvbÎncă nu există evaluări
- Module 3-4: Writing Argumentative Essay - Page - 1Document28 paginiModule 3-4: Writing Argumentative Essay - Page - 1Jan Den Saul DalanÎncă nu există evaluări
- Ensuring Patient Comfort and Clinical Accuracy During Impression Taking 3Document11 paginiEnsuring Patient Comfort and Clinical Accuracy During Impression Taking 3Raul HernandezÎncă nu există evaluări
- Role of Nurse Hospitalized ChildDocument29 paginiRole of Nurse Hospitalized ChildAjay Remya100% (2)
- 03 - Neonatal Intestinal ObstructionDocument28 pagini03 - Neonatal Intestinal Obstructionmahmoud khaledÎncă nu există evaluări
- Tuansi-Pa ManuscriptDocument11 paginiTuansi-Pa Manuscriptallkhusairy6tuansiÎncă nu există evaluări
- Research Article: An Effective LSTM Recurrent Network To Detect Arrhythmia On Imbalanced ECG DatasetDocument11 paginiResearch Article: An Effective LSTM Recurrent Network To Detect Arrhythmia On Imbalanced ECG DatasettestÎncă nu există evaluări
- M&E Training ManualDocument45 paginiM&E Training Manualsheittie100% (1)
- Laboratory Exercise No. 10 Endocrine SystemDocument3 paginiLaboratory Exercise No. 10 Endocrine SystemJamesanne DemetriaÎncă nu există evaluări
- CA Scal Provider DirectoryDocument180 paginiCA Scal Provider DirectorykevindamasoÎncă nu există evaluări
- Laporan Praktikum Faal Aplikasi PDFDocument13 paginiLaporan Praktikum Faal Aplikasi PDFSilvi ApreliaÎncă nu există evaluări
- The Effects of Covid 19 To BusinessesDocument3 paginiThe Effects of Covid 19 To BusinessesMark PadernalÎncă nu există evaluări
- My Reflection On Social MediaDocument6 paginiMy Reflection On Social MediaJoshua AladenikaÎncă nu există evaluări
- Research Paper 2Document10 paginiResearch Paper 2api-519871927Încă nu există evaluări
- 26Document5 pagini26Dr-Sanjay SinghaniaÎncă nu există evaluări
- Econometric Analysis of Health DataDocument231 paginiEconometric Analysis of Health DataMarisela FuentesÎncă nu există evaluări
- Samir 10.1007 - s11046-014-9845-2Document7 paginiSamir 10.1007 - s11046-014-9845-2قصوري سميرÎncă nu există evaluări
- Cebu City Medical Center-College of NursingDocument5 paginiCebu City Medical Center-College of NursingJimnah Rhodrick BontilaoÎncă nu există evaluări
- W 26882Document53 paginiW 26882Jose GueraÎncă nu există evaluări
- Rupture UterusDocument20 paginiRupture UterusGOODE ALBERTÎncă nu există evaluări
- Stroke AHA GuidelinesDocument104 paginiStroke AHA GuidelinesCristina ZeamaÎncă nu există evaluări