S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- EXEUNT - EZB Plant Discovery Guide - PagesDocument14 paginiEXEUNT - EZB Plant Discovery Guide - PagesGabriel Alfredo Godoy SandovalÎncă nu există evaluări
- Suturing TechniquesDocument6 paginiSuturing TechniquesAldo TanÎncă nu există evaluări
- Gynecology PDFDocument537 paginiGynecology PDFCrystal Nguyen100% (1)
- 180 Days IAS Prelims Study Plan For 2017 Prelims PDFDocument9 pagini180 Days IAS Prelims Study Plan For 2017 Prelims PDFsudhir_kumar_33Încă nu există evaluări
- Lecture notes-biochemistry-1-AAs-proteins-webDocument29 paginiLecture notes-biochemistry-1-AAs-proteins-webadane aynalem100% (1)
- HybridizationDocument19 paginiHybridizationSamer EhabÎncă nu există evaluări
- Disseminated Intravascular CoagulationDocument19 paginiDisseminated Intravascular CoagulationAnna MilliziaÎncă nu există evaluări
- Low-Density Lipoprotein Subclass Distribution PatternDocument8 paginiLow-Density Lipoprotein Subclass Distribution PatternOlfiany Laurenzia PongohÎncă nu există evaluări
- 0809 03eDocument5 pagini0809 03eOlfiany Laurenzia PongohÎncă nu există evaluări
- Acute Lymphoblastic LeukemiaDocument14 paginiAcute Lymphoblastic LeukemiaOlfiany Laurenzia PongohÎncă nu există evaluări
- Human Cytotrofoblas Diferentiation PDFDocument10 paginiHuman Cytotrofoblas Diferentiation PDFOlfiany Laurenzia PongohÎncă nu există evaluări
- Severe Sepsis and Septic Shock - RiversDocument28 paginiSevere Sepsis and Septic Shock - RiversMihai SalceanuÎncă nu există evaluări
- Cancer Stem CellsDocument9 paginiCancer Stem CellsOlfiany Laurenzia PongohÎncă nu există evaluări
- General: Anaemia & Blood Cell Transfusion in Critical IllnessDocument1 paginăGeneral: Anaemia & Blood Cell Transfusion in Critical IllnessOlfiany Laurenzia PongohÎncă nu există evaluări
- StemiDocument2 paginiStemiOlfiany Laurenzia PongohÎncă nu există evaluări
- Thrombomodulin Tumour Biology and PrognosticDocument4 paginiThrombomodulin Tumour Biology and PrognosticOlfiany Laurenzia PongohÎncă nu există evaluări
- A Candidate Gene Study of Folate-Associated One CarbonDocument18 paginiA Candidate Gene Study of Folate-Associated One CarbonOlfiany Laurenzia PongohÎncă nu există evaluări
- The Relationship Between Serum Adiponectin Levels With TheDocument6 paginiThe Relationship Between Serum Adiponectin Levels With TheOlfiany Laurenzia PongohÎncă nu există evaluări
- Uc MGP Biomarker For CVDDocument10 paginiUc MGP Biomarker For CVDOlfiany Laurenzia PongohÎncă nu există evaluări
- Neonatal Hyperbilirubinemia and Elevated Liver Enzymes Associated With Thyroid Hormone Deficiency in NeonatesDocument4 paginiNeonatal Hyperbilirubinemia and Elevated Liver Enzymes Associated With Thyroid Hormone Deficiency in NeonatesOlfiany Laurenzia PongohÎncă nu există evaluări
- A 68-Year-Old Man With Thrombocytosis and Ringed Sideroblasts (Sukma) - 3Document2 paginiA 68-Year-Old Man With Thrombocytosis and Ringed Sideroblasts (Sukma) - 3Olfiany Laurenzia PongohÎncă nu există evaluări
- Laboratory Evaluation of Coagulation Inhibitors (Endang)Document5 paginiLaboratory Evaluation of Coagulation Inhibitors (Endang)Olfiany Laurenzia Pongoh100% (1)
- Apoptoza Boli DegenerativeDocument11 paginiApoptoza Boli DegenerativeDiana IordacheÎncă nu există evaluări
- Hipolatamik AmenoreaDocument11 paginiHipolatamik AmenoreaRai Tunggal IsmayaÎncă nu există evaluări
- AIS Case BagusDocument7 paginiAIS Case BagusOlfiany Laurenzia PongohÎncă nu există evaluări
- A Case of Aspartate Aminotransferase MacroenzymeDocument3 paginiA Case of Aspartate Aminotransferase MacroenzymeOlfiany Laurenzia PongohÎncă nu există evaluări
- Caffeinated Coffee Does Not Acutely AffectDocument5 paginiCaffeinated Coffee Does Not Acutely AffectOlfiany Laurenzia PongohÎncă nu există evaluări
- Hemostasis HandbookDocument36 paginiHemostasis HandbookWilhelm HeinleinÎncă nu există evaluări
- IiiiiiDocument8 paginiIiiiiiAyusriwahyuni RambeÎncă nu există evaluări
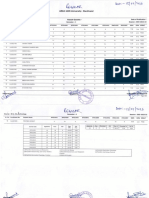
- Result Gazette Regular ODD 22 23 1st Semester B.SC Biotechnology. 1Document2 paginiResult Gazette Regular ODD 22 23 1st Semester B.SC Biotechnology. 1Abhishek BhaduriÎncă nu există evaluări
- National Grade Six Assessment ScienceDocument11 paginiNational Grade Six Assessment ScienceGrace EtwaruÎncă nu există evaluări
- Niko Tinbergen and The Red Patch On The Herring Gull's BeakDocument10 paginiNiko Tinbergen and The Red Patch On The Herring Gull's BeakchurianaÎncă nu există evaluări
- MCU Mata Cristy MaeDocument14 paginiMCU Mata Cristy MaeJean JacquesÎncă nu există evaluări
- 2010 Lennette's - Laboratory - Diagnosis PDFDocument512 pagini2010 Lennette's - Laboratory - Diagnosis PDFHumberto Azuara Jiménez100% (1)
- Growth Response of Moringa Oleifera (Lam) To Water Stress and To Arid Bioclimatic ConditionsDocument11 paginiGrowth Response of Moringa Oleifera (Lam) To Water Stress and To Arid Bioclimatic Conditionsυκοντχου ΛεχρανδÎncă nu există evaluări
- Habitat and Adaptation - Grade 5Document6 paginiHabitat and Adaptation - Grade 5Rasha GhabbounÎncă nu există evaluări
- Grade 7 Science Cells in Its EnvironmentDocument14 paginiGrade 7 Science Cells in Its Environmentapi-235404570100% (1)
- Ex 2 Protein DenaturationDocument4 paginiEx 2 Protein DenaturationDaniel Seth AndalÎncă nu există evaluări
- Etymology: Meros Meaning "Part". The Term Was Coined in 1833 by Jöns Jacob Berzelius, Although HisDocument12 paginiEtymology: Meros Meaning "Part". The Term Was Coined in 1833 by Jöns Jacob Berzelius, Although HisZoya KapoorÎncă nu există evaluări
- Gathfan Tsaqif Prasetya - Rsu - BundaDocument1 paginăGathfan Tsaqif Prasetya - Rsu - BundaBunk ZoelÎncă nu există evaluări
- BIOLOGYDocument2 paginiBIOLOGYMyraSimoraÎncă nu există evaluări
- Soy Sauce Production FinalDocument40 paginiSoy Sauce Production Finalafidah99Încă nu există evaluări
- Soma Devi InvoiceDocument1 paginăSoma Devi InvoiceManeesh Verma100% (1)
- 1 s2.0 S2213576613000808 MainDocument2 pagini1 s2.0 S2213576613000808 MainUmi AndikaÎncă nu există evaluări
- Mitosis Internet LessonDocument3 paginiMitosis Internet LessonGLENMAR VINEGASÎncă nu există evaluări
- Bioinformatics PDFDocument336 paginiBioinformatics PDFJoel CordeiroÎncă nu există evaluări
- Immunofluorescence Tests: Direct and IndirectDocument489 paginiImmunofluorescence Tests: Direct and IndirectmeskiÎncă nu există evaluări
- Botany Assignment 1 PDFDocument11 paginiBotany Assignment 1 PDFSyed Haider Ali Shah SheraziÎncă nu există evaluări
- Planj Bio t4Document303 paginiPlanj Bio t4Nur Anida IsmailÎncă nu există evaluări
- Lecture 3 Genetic CounselingDocument23 paginiLecture 3 Genetic Counselingimorkzone100% (1)
- January 2018Document4 paginiJanuary 2018Athula Dias NagahawatteÎncă nu există evaluări