S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Perfume Formulation Technology Hand BookDocument16 paginiPerfume Formulation Technology Hand BookFaltumsg30% (10)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
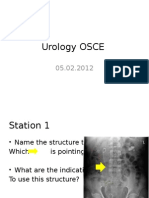
- Urology OSCE: Radiological AbnormalitiesDocument9 paginiUrology OSCE: Radiological AbnormalitiesJihad Anad75% (4)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Aleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Document14 paginiAleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Jihad AnadÎncă nu există evaluări
- Manual of Urology - Diagnosis & Therapy (2nd Ed.)Document362 paginiManual of Urology - Diagnosis & Therapy (2nd Ed.)Alina Ghe100% (3)
- Proteccion Contra Sobretensiones PDFDocument84 paginiProteccion Contra Sobretensiones PDFgilbertomjcÎncă nu există evaluări
- Analytical Methods To Measure The Constants of Fats and OilsDocument5 paginiAnalytical Methods To Measure The Constants of Fats and OilsPenicillium Notatum67% (3)
- Manual de Uso Ecografo GE Logiq e PDFDocument192 paginiManual de Uso Ecografo GE Logiq e PDFDaniel CortesÎncă nu există evaluări
- 4 5879809992000800192 PDFDocument323 pagini4 5879809992000800192 PDFJihad AnadÎncă nu există evaluări
- Git Contrast Study1Document29 paginiGit Contrast Study1Jihad AnadÎncă nu există evaluări
- Irrigating Fluids in Endoscopic Surgery: ReviewDocument12 paginiIrrigating Fluids in Endoscopic Surgery: ReviewJihad AnadÎncă nu există evaluări
- Ultrasound NotesDocument19 paginiUltrasound NotesJihad Anad100% (1)
- Urology Slides: DR - JihadDocument4 paginiUrology Slides: DR - JihadJihad Anad100% (1)
- WJCC 3 245Document21 paginiWJCC 3 245Jihad AnadÎncă nu există evaluări
- Van de Graaff GeneratorDocument10 paginiVan de Graaff GeneratorJihad AnadÎncă nu există evaluări
- Dr. Anad's Guide to Urosepsis: Causes, Symptoms and TreatmentDocument23 paginiDr. Anad's Guide to Urosepsis: Causes, Symptoms and TreatmentJihad Anad100% (1)
- Kundalini Yoga & MeditationDocument123 paginiKundalini Yoga & MeditationFejes Zoltan100% (4)
- Urology Slides: DR - JihadDocument4 paginiUrology Slides: DR - JihadJihad Anad100% (1)
- Ultrasound NotesDocument19 paginiUltrasound NotesJihad Anad100% (1)
- Gaur Et Al-2002-BJU InternationalDocument5 paginiGaur Et Al-2002-BJU InternationalJihad AnadÎncă nu există evaluări
- Kundalini Yoga & MeditationDocument123 paginiKundalini Yoga & MeditationFejes Zoltan100% (4)
- Urethral BulkingDocument7 paginiUrethral BulkingJihad AnadÎncă nu există evaluări
- CHA3545 Periurethral Bulking Agent PEDocument10 paginiCHA3545 Periurethral Bulking Agent PEJihad AnadÎncă nu există evaluări
- Answer For Urology MCQDocument1 paginăAnswer For Urology MCQJihad AnadÎncă nu există evaluări
- JSCFE Guidance Notes For Referees - GenericDocument2 paginiJSCFE Guidance Notes For Referees - GenericJihad AnadÎncă nu există evaluări
- Testicular Cancer Staging and Treatment GuideDocument58 paginiTesticular Cancer Staging and Treatment GuideJihad AnadÎncă nu există evaluări
- JSCFE Guidance Notes For Applicants - GenericDocument2 paginiJSCFE Guidance Notes For Applicants - GenericJihad AnadÎncă nu există evaluări
- Hacking Made Easy by Dr. Robot and Hacking UniversityDocument47 paginiHacking Made Easy by Dr. Robot and Hacking UniversityJihad AnadÎncă nu există evaluări
- Antibiotics: by Dr. Jihad AnadDocument89 paginiAntibiotics: by Dr. Jihad AnadJihad AnadÎncă nu există evaluări
- DiureticsDocument6 paginiDiureticsJihad AnadÎncă nu există evaluări
- Penile prosthesis improves quality of lifeDocument4 paginiPenile prosthesis improves quality of lifeJihad AnadÎncă nu există evaluări
- PCNL EeDocument6 paginiPCNL EeJihad AnadÎncă nu există evaluări
- Penile Prosthes OutcomesDocument42 paginiPenile Prosthes OutcomesJihad AnadÎncă nu există evaluări
- Tyco TY8281 TFP680 - 03 - 2023Document17 paginiTyco TY8281 TFP680 - 03 - 2023First LAstÎncă nu există evaluări
- Chinkon Kishin - Origens Shintoístas Do Okiyome e Do Espiritismo Na MahikariDocument2 paginiChinkon Kishin - Origens Shintoístas Do Okiyome e Do Espiritismo Na MahikariGauthier Alex Freitas de Abreu0% (1)
- Preparation and Evaluation of Orthodontic Setup PDFDocument20 paginiPreparation and Evaluation of Orthodontic Setup PDFLiezty VioLen'sÎncă nu există evaluări
- General Guidelines For Design and Construction of Concrete Diaphram (Slurry) WallsDocument108 paginiGeneral Guidelines For Design and Construction of Concrete Diaphram (Slurry) WallsharleyÎncă nu există evaluări
- Grade 9 Unit 1 - Part 1: Square RootsDocument20 paginiGrade 9 Unit 1 - Part 1: Square RootsWilson ZhangÎncă nu există evaluări
- BS 7941-1-2006Document20 paginiBS 7941-1-2006Willy AryansahÎncă nu există evaluări
- 25f8e d64fDocument6 pagini25f8e d64fapi-233604231Încă nu există evaluări
- Indian War of Independence 1857 - Part 2Document150 paginiIndian War of Independence 1857 - Part 2BISWAJIT MOHANTYÎncă nu există evaluări
- Radiesse Pálpebras Gox-8-E2633Document7 paginiRadiesse Pálpebras Gox-8-E2633Camila CrosaraÎncă nu există evaluări
- Research Article (Lavandula Angustifolia) Essential Oil On: Effect of Lavender Acute Inflammatory ResponseDocument10 paginiResearch Article (Lavandula Angustifolia) Essential Oil On: Effect of Lavender Acute Inflammatory ResponseAndreeaÎncă nu există evaluări
- Welding Defects and AcceptanceDocument76 paginiWelding Defects and Acceptancearavindan100% (1)
- Student Pilot GuideDocument13 paginiStudent Pilot GuideAŞKIN FIRATÎncă nu există evaluări
- Minicargador Cat 246Document22 paginiMinicargador Cat 246Juanca FerroÎncă nu există evaluări
- Dr. Carlos S. Lanting College: College of Maritime EducationDocument14 paginiDr. Carlos S. Lanting College: College of Maritime EducationJeynard Moler J. TanÎncă nu există evaluări
- DA1 Learning - Ans KeyDocument4 paginiDA1 Learning - Ans KeyDolon DasÎncă nu există evaluări
- Operating Systems: Chapter 3: DeadlocksDocument46 paginiOperating Systems: Chapter 3: DeadlocksManoel Katlib100% (1)
- 2021 Vallourec Universal Registration DocumentDocument368 pagini2021 Vallourec Universal Registration DocumentRolando Jara YoungÎncă nu există evaluări
- GBDocument10 paginiGBQuoctytranÎncă nu există evaluări
- WHO Blocks Nanosilver Shipments to Treat Ebola in AfricaDocument2 paginiWHO Blocks Nanosilver Shipments to Treat Ebola in AfricaTamas ZefferÎncă nu există evaluări
- SEFT Islamic care effect on hypertension patients' blood pressureDocument12 paginiSEFT Islamic care effect on hypertension patients' blood pressureSopian HadiÎncă nu există evaluări
- General Biology 2: Quarter 3, Module 1 Genetic EngineeringDocument20 paginiGeneral Biology 2: Quarter 3, Module 1 Genetic EngineeringRonalyn AndaganÎncă nu există evaluări
- Telemark PulloverDocument2 paginiTelemark Pulloverkidknits100% (1)
- Mic ProjectDocument12 paginiMic Projectsarthakjoshi012Încă nu există evaluări
- WIP CaseStudyDocument3 paginiWIP CaseStudypaul porrasÎncă nu există evaluări
- Sherco 450 Se R Workshop Manual 1Document79 paginiSherco 450 Se R Workshop Manual 1miguelÎncă nu există evaluări
- Conflict and Factional Disputes - Siegel & BealsDocument12 paginiConflict and Factional Disputes - Siegel & BealsDanielÎncă nu există evaluări
- Organization Structure Training KAJARIADocument30 paginiOrganization Structure Training KAJARIAViswanth GanaparthiÎncă nu există evaluări