S-ar putea să vă placă și
- Biopsy in Oral SurgeryDocument45 paginiBiopsy in Oral SurgeryMahamoud IsmailÎncă nu există evaluări
- 973 3641 1 PBDocument1 pagină973 3641 1 PBAamir BugtiÎncă nu există evaluări
- B5 Guide Cover Art (Ol) .Indd 1 11/5/05 11:05:33 AM 11/5/05 11:05:33 AMDocument158 paginiB5 Guide Cover Art (Ol) .Indd 1 11/5/05 11:05:33 AM 11/5/05 11:05:33 AMAamir BugtiÎncă nu există evaluări
- Textbook List - Semester 1 2016Document3 paginiTextbook List - Semester 1 2016Aamir BugtiÎncă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Endo Flare UpDocument25 paginiEndo Flare UpAamir BugtiÎncă nu există evaluări
- Pregnancy Precautions in Dental Clinic: Pregnancy Myth: A Mother Loses A Tooth For Every BabyDocument17 paginiPregnancy Precautions in Dental Clinic: Pregnancy Myth: A Mother Loses A Tooth For Every BabyAamir BugtiÎncă nu există evaluări
- Anatomy of A Case Study: AdvantagesDocument1 paginăAnatomy of A Case Study: AdvantagesAnonymous ihOnWWlHQÎncă nu există evaluări
- Perio Article PDFDocument4 paginiPerio Article PDFAamir BugtiÎncă nu există evaluări
- BiostatsDocument35 paginiBiostatsAamir BugtiÎncă nu există evaluări
- Complication in Dental ChairDocument25 paginiComplication in Dental ChairAamir BugtiÎncă nu există evaluări
- A e Me Membership FormDocument5 paginiA e Me Membership FormAamir BugtiÎncă nu există evaluări
- Basic Surgical InstrumentsDocument26 paginiBasic Surgical InstrumentsJun ManÎncă nu există evaluări
- Public Health Administration ReviewDocument9 paginiPublic Health Administration Reviewpolitronxx0% (1)
- Cohort StudiesDocument79 paginiCohort StudiesAamir BugtiÎncă nu există evaluări
- Management of Highly Resorbed Mandibular RidgeDocument11 paginiManagement of Highly Resorbed Mandibular RidgeAamir BugtiÎncă nu există evaluări
- Novel Registration Technique To Register Neutral ZoneDocument5 paginiNovel Registration Technique To Register Neutral ZoneAamir BugtiÎncă nu există evaluări
- Neutral Zone Approach For Severely Atrophic RidgesDocument5 paginiNeutral Zone Approach For Severely Atrophic RidgesAamir Bugti100% (1)
- Novel Registration Technique To Register Neutral ZoneDocument5 paginiNovel Registration Technique To Register Neutral ZoneAamir BugtiÎncă nu există evaluări
- Mood StabilizersDocument4 paginiMood StabilizersAamir BugtiÎncă nu există evaluări
- Impression Techniques For The ResorbedDocument4 paginiImpression Techniques For The ResorbedAamir BugtiÎncă nu există evaluări
- Prosthodontic Management of Severely ResorbedDocument2 paginiProsthodontic Management of Severely ResorbedAamir BugtiÎncă nu există evaluări
- Merkblatt EngDocument2 paginiMerkblatt EngMuhammed Talha QureshiÎncă nu există evaluări
- GoutDocument4 paginiGoutAamir BugtiÎncă nu există evaluări
- Compare Prokaryotes and Eukaryotes: Gram +ve Gram - Ve Peptidoglycan Layer Teichoic Acid Surface AntigenDocument12 paginiCompare Prokaryotes and Eukaryotes: Gram +ve Gram - Ve Peptidoglycan Layer Teichoic Acid Surface AntigenAamir BugtiÎncă nu există evaluări
- Mnemonic SDocument4 paginiMnemonic SAamir BugtiÎncă nu există evaluări
- Microbiology2 EnumerateDocument14 paginiMicrobiology2 EnumerateAamir BugtiÎncă nu există evaluări
- Introduction To Medical VirologyDocument5 paginiIntroduction To Medical VirologyAamir BugtiÎncă nu există evaluări
- DepressionDocument9 paginiDepressionAamir BugtiÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Plac908 Dap Record 5 2023Document3 paginiPlac908 Dap Record 5 2023api-706977810Încă nu există evaluări
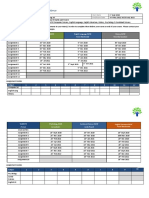
- AlOmar, Dalal - Assignment ScheduleDocument4 paginiAlOmar, Dalal - Assignment ScheduleDalal AlomarÎncă nu există evaluări
- Dialogue Oral On Handphone TopicDocument2 paginiDialogue Oral On Handphone Topicsuriya ars75% (81)
- Department: Uils: Environmental Law & Wildlife Protection Amanat Kahlon Assistant Professor Chandigarh UniversityDocument7 paginiDepartment: Uils: Environmental Law & Wildlife Protection Amanat Kahlon Assistant Professor Chandigarh UniversityHarneet KaurÎncă nu există evaluări
- Cannon-Ball Engineering: (Consulting Engineers)Document2 paginiCannon-Ball Engineering: (Consulting Engineers)isaacjoe77100% (1)
- A Hybrid Approach For Face Recognition Using A Convolutional Neural Network Combined With Feature Extraction TechniquesDocument14 paginiA Hybrid Approach For Face Recognition Using A Convolutional Neural Network Combined With Feature Extraction TechniquesIAES IJAIÎncă nu există evaluări
- 2 Story Telling Templetes 2023Document1 pagină2 Story Telling Templetes 2023serkovanastya12Încă nu există evaluări
- 09 Measures of VariabilityDocument15 pagini09 Measures of VariabilityReina100% (1)
- A3 DomainModelingDocument5 paginiA3 DomainModelingJaspreet Singh SidhuÎncă nu există evaluări
- KG 2 1Document10 paginiKG 2 1prashantkumar1lifeÎncă nu există evaluări
- Introduction: Digital Controller Design: SystemDocument13 paginiIntroduction: Digital Controller Design: Systembala_aeroÎncă nu există evaluări
- Optimus Prime - : Age of ExtinctionDocument4 paginiOptimus Prime - : Age of ExtinctionDaniel Leon AlcaÎncă nu există evaluări
- The Impact of Brands On Consumer PurchasDocument6 paginiThe Impact of Brands On Consumer PurchasKovai MTÎncă nu există evaluări
- Assignment Brief Course No.:: 010303100: Functional MathematicsDocument10 paginiAssignment Brief Course No.:: 010303100: Functional MathematicsEng-Mohammed TwiqatÎncă nu există evaluări
- IUCAA ReportDocument4 paginiIUCAA ReportRADHIKA BHARADIYAÎncă nu există evaluări
- Tps 22967Document29 paginiTps 22967Thanh LeeÎncă nu există evaluări
- American Accounting AssociationDocument13 paginiAmerican Accounting AssociationRahmat Pasaribu OfficialÎncă nu există evaluări
- Legaledge Test Series: Mock Common Law Admission Test 2024 Mock Clat - 03Document40 paginiLegaledge Test Series: Mock Common Law Admission Test 2024 Mock Clat - 03Ashutosh MalviyaÎncă nu există evaluări
- MSC 2011-10S370Document70 paginiMSC 2011-10S370caraiane100% (2)
- Full Download Test Bank For Public Health Nursing 10th Edition Stanhope PDF Full ChapterDocument36 paginiFull Download Test Bank For Public Health Nursing 10th Edition Stanhope PDF Full Chaptertheresagreensayxgiwkod100% (18)
- Session 4 Stephanie CicchiniDocument20 paginiSession 4 Stephanie CicchiniMarinos GounaridisÎncă nu există evaluări
- Dragline Cycle TimeDocument11 paginiDragline Cycle TimeanfiboleÎncă nu există evaluări
- Project 2020 1 IT02 KA229 079474Document3 paginiProject 2020 1 IT02 KA229 079474RECAİ TAŞÎncă nu există evaluări
- Article Nejib SeismoDocument25 paginiArticle Nejib SeismoseimedÎncă nu există evaluări
- EP Printables: Levels 1-4: Earth ScienceDocument35 paginiEP Printables: Levels 1-4: Earth ScienceArle CambalÎncă nu există evaluări
- Film Art Study Guide Key TermsDocument8 paginiFilm Art Study Guide Key TermsnormanchamorroÎncă nu există evaluări
- Chandramohan (2016) Duration (Stanford) PDFDocument448 paginiChandramohan (2016) Duration (Stanford) PDFmgrubisicÎncă nu există evaluări
- BBA Lecture NotesDocument36 paginiBBA Lecture NotesSaqib HanifÎncă nu există evaluări
- Assessment in Special EdDocument27 paginiAssessment in Special EdAlfred IntongÎncă nu există evaluări
- Chapter 3 Resurvey and Verification SurveyDocument18 paginiChapter 3 Resurvey and Verification SurveyNaqibDarwishÎncă nu există evaluări