S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Anatomy of Womans Sex OrganDocument5 paginiAnatomy of Womans Sex Organsumeer khan63% (8)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Figures & Boxes of Davidson's Medicine (Paper I) - Acc. To FCPS SyllabusDocument202 paginiFigures & Boxes of Davidson's Medicine (Paper I) - Acc. To FCPS SyllabusHasibul Hassan Shanto50% (2)
- Notes For Perioperative NursingDocument5 paginiNotes For Perioperative NursingNey JuneÎncă nu există evaluări
- Hospitals That Offer ObservershipsDocument6 paginiHospitals That Offer ObservershipsNisarg DaveÎncă nu există evaluări
- White Spot LesionsDocument8 paginiWhite Spot LesionsMicéli Guimarães BlayaÎncă nu există evaluări
- Versana Essential Transducer Guide CompleteDocument2 paginiVersana Essential Transducer Guide CompleteHelmi Agustian100% (4)
- Basic Concepts in Pregnancy: Prenatal Care and Health TeachingsDocument12 paginiBasic Concepts in Pregnancy: Prenatal Care and Health Teachingswanda100% (2)
- Health Family Welfare 3Document225 paginiHealth Family Welfare 3Gopala Sundararaj SÎncă nu există evaluări
- Priority Nursing Actions Allen's TestDocument6 paginiPriority Nursing Actions Allen's Testwanda100% (2)
- 7 Ps of Service Marketing Apollo HospitalDocument18 pagini7 Ps of Service Marketing Apollo HospitalManish ManjhiÎncă nu există evaluări
- HELLP Concept Map RevisedDocument1 paginăHELLP Concept Map RevisedwandaÎncă nu există evaluări
- Maternal & Child NursingDocument10 paginiMaternal & Child Nursingnokolip100% (2)
- PDFDocument7 paginiPDFwandaÎncă nu există evaluări
- Claim Form (Out Patient + Hospitalisation)Document2 paginiClaim Form (Out Patient + Hospitalisation)ahsan_hayat28660% (1)
- Pocket-Book MCH Emergencies - English PDFDocument286 paginiPocket-Book MCH Emergencies - English PDFAbigail Kusi-Amponsah100% (1)
- The Language of Anatomy: ExerciseDocument14 paginiThe Language of Anatomy: Exercisewn4tb100% (1)
- Approach To Skin Adnexal TumorsDocument20 paginiApproach To Skin Adnexal TumorsNirmalya Chakrabarti100% (1)
- Latihan Soal Koding Semester 4Document3 paginiLatihan Soal Koding Semester 4kamilaÎncă nu există evaluări
- Sinus Lift ChenDocument10 paginiSinus Lift ChenCarlos Frederico Nunes PavãoÎncă nu există evaluări
- Consent TATDocument1 paginăConsent TATryanash777Încă nu există evaluări
- Drop Foot, An Unexpected Complication of Vaginal HysterectomyDocument4 paginiDrop Foot, An Unexpected Complication of Vaginal HysterectomySandraSaracÎncă nu există evaluări
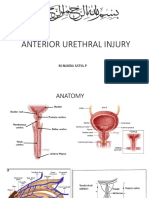
- Rupture Urethra Anterior DR Sule FixDocument36 paginiRupture Urethra Anterior DR Sule FixkadinfathiaÎncă nu există evaluări
- Sulci and GyriDocument24 paginiSulci and GyriravigoaÎncă nu există evaluări
- UEU-Undergraduate-13928-DAFTAR PUSTAKA - Image.MarkedDocument4 paginiUEU-Undergraduate-13928-DAFTAR PUSTAKA - Image.MarkedAlif Akbar HasyimiÎncă nu există evaluări
- Amenorrhea Ovarian TumorsDocument18 paginiAmenorrhea Ovarian TumorsJeremy ShimlerÎncă nu există evaluări
- Medical CertificateDocument27 paginiMedical CertificatemarizamoraÎncă nu există evaluări
- Sebaceous CystDocument4 paginiSebaceous CystristaniatauhidÎncă nu există evaluări
- Unit 3 Hospital Staffs and Departments: Objectives: After The Lesson, Students Will Be Able ToDocument22 paginiUnit 3 Hospital Staffs and Departments: Objectives: After The Lesson, Students Will Be Able ToLinh TrầnÎncă nu există evaluări
- Pathophysiology and Management of TTN-2020Document11 paginiPathophysiology and Management of TTN-2020JerlonÎncă nu există evaluări
- Magna Carta of Women Leave PrivilegesDocument35 paginiMagna Carta of Women Leave PrivilegesMari DjoÎncă nu există evaluări
- CHN Notes For MidtermsDocument24 paginiCHN Notes For MidtermsReiner Lopez100% (1)
- D1 - Theraputic Guidelines in Neonatal InfectionDocument15 paginiD1 - Theraputic Guidelines in Neonatal InfectiongaasheÎncă nu există evaluări
- VAC Diversified FlowDocument1 paginăVAC Diversified FlowWinnie AtienoÎncă nu există evaluări
- Session 4Document17 paginiSession 4Dian Indra YuniartoÎncă nu există evaluări