S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Jadwal Follow Up 2Document1 paginăJadwal Follow Up 2pebrianiiiiÎncă nu există evaluări
- Jadwal Follow Up Stase Digestif 26-31 Januari 2015Document1 paginăJadwal Follow Up Stase Digestif 26-31 Januari 2015pebrianiiiiÎncă nu există evaluări
- Daftar PustakaDocument1 paginăDaftar PustakapebrianiiiiÎncă nu există evaluări
- Anemia Chronic DiseaseDocument2 paginiAnemia Chronic DiseasepebrianiiiiÎncă nu există evaluări
- DMB 3677Document23 paginiDMB 3677pebrianiiiiÎncă nu există evaluări
- Daftar PustakaDocument1 paginăDaftar PustakaAchmad FitrahÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
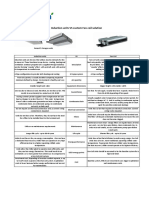
- HotelSolution: Induction Units VS Fan-Coil SolutionDocument1 paginăHotelSolution: Induction Units VS Fan-Coil SolutionMoriyasu NguyenÎncă nu există evaluări
- Flux 10 4 New Features Presentation ValideDocument22 paginiFlux 10 4 New Features Presentation ValideleelÎncă nu există evaluări
- HP Officejet Pro X476 X576 TroubleshootingDocument152 paginiHP Officejet Pro X476 X576 Troubleshootingjason7493Încă nu există evaluări
- Chemical BondingDocument6 paginiChemical BondingNoongju AbdullahÎncă nu există evaluări
- Chapter 3 Dynamics of Robotics SystemDocument38 paginiChapter 3 Dynamics of Robotics SystemAddisuSaafooÎncă nu există evaluări
- Unit Hydrograph DerivationDocument7 paginiUnit Hydrograph DerivationSudharsananPRSÎncă nu există evaluări
- Thermal Engineering PDFDocument76 paginiThermal Engineering PDFKartik KuriÎncă nu există evaluări
- 2019 Hydropower Status Report 0Document56 pagini2019 Hydropower Status Report 0Titos Nicosio ComéÎncă nu există evaluări
- Materials I: Lecture Course 5 Phase Diagrams. Fe-C Diagram. Crystallisation of Alloys in Fe - Fe C SystemDocument24 paginiMaterials I: Lecture Course 5 Phase Diagrams. Fe-C Diagram. Crystallisation of Alloys in Fe - Fe C SystemTiger ClaudiuÎncă nu există evaluări
- HW2 Solutions FinalDocument5 paginiHW2 Solutions Finalpande_100Încă nu există evaluări
- Improve Steel Quality with Electromagnetic StirrersDocument4 paginiImprove Steel Quality with Electromagnetic Stirrerst_pradipÎncă nu există evaluări
- Formulae and Design Rules To Ec2Document45 paginiFormulae and Design Rules To Ec2moodoo100% (4)
- 1 Design Basis 1.1 Material and Properties 1.1 Material and PropertiesDocument13 pagini1 Design Basis 1.1 Material and Properties 1.1 Material and PropertiesDarshan PanchalÎncă nu există evaluări
- Applications of Nano Biotechnology in Wastewater Treatment PDFDocument9 paginiApplications of Nano Biotechnology in Wastewater Treatment PDFswaroop_exlncÎncă nu există evaluări
- Chapter 4: Dynamics: Force and Newton'S Laws of Motion: Net F Ma (63.0 KG) (4.20 M/s ) 265 NDocument15 paginiChapter 4: Dynamics: Force and Newton'S Laws of Motion: Net F Ma (63.0 KG) (4.20 M/s ) 265 NCedric KouakouÎncă nu există evaluări
- Latent Print DevelopmentDocument20 paginiLatent Print Developmentapi-272036460100% (1)
- Quantum NumbersDocument10 paginiQuantum Numbersaplattinum1633Încă nu există evaluări
- Air Preheater Technical PaperDocument21 paginiAir Preheater Technical Paperchekoti koushikÎncă nu există evaluări
- Department of Education: Humss 12 Cluster A and B Weekly Home Learning PlanDocument3 paginiDepartment of Education: Humss 12 Cluster A and B Weekly Home Learning PlanRhomelyn AbellarÎncă nu există evaluări
- Energy in Somaliland Novia Thesis - Editing PDFDocument25 paginiEnergy in Somaliland Novia Thesis - Editing PDFAbdirahmanÎncă nu există evaluări
- Rebound Hammer Test Procedure For Concrete HardnessDocument4 paginiRebound Hammer Test Procedure For Concrete HardnessSite Engineer.2p2Încă nu există evaluări
- Cup Making MachineDocument3 paginiCup Making MachineJournalNX - a Multidisciplinary Peer Reviewed JournalÎncă nu există evaluări
- Schrodinger Equation DerivationDocument12 paginiSchrodinger Equation DerivationAndrés López Martínez100% (1)
- Hvs-313. Maximum Demand ControllerDocument3 paginiHvs-313. Maximum Demand ControllerHari BabuÎncă nu există evaluări
- SABIC Innovative Plastics Lexan® 940 PC Data SheetDocument3 paginiSABIC Innovative Plastics Lexan® 940 PC Data SheetMRC RailÎncă nu există evaluări
- Dane Rudhyar - The Planets and Their Symbols - MARCADODocument13 paginiDane Rudhyar - The Planets and Their Symbols - MARCADOLuiza Machado100% (2)
- Fjbzr6wn50 - Class 7 Timetable - Fua 2024Document2 paginiFjbzr6wn50 - Class 7 Timetable - Fua 2024mrs.prernajainÎncă nu există evaluări
- Printed Vesiontunable Optical Properties of Bi12Na12TiO3 Materials Via Sm12Na12TiO3Document8 paginiPrinted Vesiontunable Optical Properties of Bi12Na12TiO3 Materials Via Sm12Na12TiO3Vinh PhamÎncă nu există evaluări
- Aspect ManualDocument444 paginiAspect ManualArijit LaikÎncă nu există evaluări
- Signal TransductionDocument33 paginiSignal TransductiongilmeanualexmihaiÎncă nu există evaluări