S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Healthy KetosysIntermittent FastingDocument64 paginiHealthy KetosysIntermittent Fastingrrajen195% (20)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Diabetes and Diabetic DietDocument4 paginiDiabetes and Diabetic DietSereneOne50% (2)
- Oncologic EmergenciesDocument32 paginiOncologic EmergenciesDemocrito Louierick Plaza VI100% (1)
- Sheri Colberg - The Diabetic Athlete (2001, Human Kinetics)Document276 paginiSheri Colberg - The Diabetic Athlete (2001, Human Kinetics)Vijay DhamuÎncă nu există evaluări
- Weight-For-Height BOYS: 2 To 5 Years (Z-Scores)Document1 paginăWeight-For-Height BOYS: 2 To 5 Years (Z-Scores)Malisa Lukman100% (1)
- Weight-For-Height BOYS: 2 To 5 Years (Z-Scores)Document1 paginăWeight-For-Height BOYS: 2 To 5 Years (Z-Scores)Malisa Lukman100% (1)
- Anesthesia NutshellDocument388 paginiAnesthesia NutshellMuhammad UmerÎncă nu există evaluări
- Roche GlucoseDocument4 paginiRoche GlucoseDiep LeÎncă nu există evaluări
- Treatment of Diabetes Dr. Osama MahmoudDocument33 paginiTreatment of Diabetes Dr. Osama Mahmoudمحيي الدين الكميشىÎncă nu există evaluări
- RefreshDocument1 paginăRefreshErenJelaluÎncă nu există evaluări
- BioetikaDocument49 paginiBioetikaErenJelaluÎncă nu există evaluări
- BioetikaDocument49 paginiBioetikaErenJelaluÎncă nu există evaluări
- CBD DR Saugi - Monika SM-30101507496Document62 paginiCBD DR Saugi - Monika SM-30101507496Novi Dian LestariÎncă nu există evaluări
- Makalah FarmakoepidemiologiDocument24 paginiMakalah FarmakoepidemiologiAkbar NugrahaÎncă nu există evaluări
- GlipizideDocument2 paginiGlipizideFeliciaDorghamÎncă nu există evaluări
- Diabetes and Exercise: When To Monitor Your Blood Sugar: by Mayo Clinic StaffDocument2 paginiDiabetes and Exercise: When To Monitor Your Blood Sugar: by Mayo Clinic StaffRatnaPrasadNalamÎncă nu există evaluări
- Diagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newDocument94 paginiDiagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newmatrix_oriÎncă nu există evaluări
- ISPAD Clinical Practice Consensus Guidelines 2018: Management of Children and Adolescents With Diabetes Requiring SurgeryDocument10 paginiISPAD Clinical Practice Consensus Guidelines 2018: Management of Children and Adolescents With Diabetes Requiring SurgeryAbdi KebedeÎncă nu există evaluări
- Nutrition Care Process NoteDocument3 paginiNutrition Care Process Noteapi-242497565Încă nu există evaluări
- 7396 PDFDocument7 pagini7396 PDFFranz BackenbauerÎncă nu există evaluări
- New Microsoft Word DocumentDocument6 paginiNew Microsoft Word DocumentKawther El-FikyÎncă nu există evaluări
- Mortality Report April 25th 2019Document12 paginiMortality Report April 25th 2019ramotÎncă nu există evaluări
- Jurnal Anastesi ImeldaDocument10 paginiJurnal Anastesi ImeldayevanharrybrataÎncă nu există evaluări
- IV Insulin Infusion ProtocolDocument4 paginiIV Insulin Infusion ProtocolWeeranan Sueb-LaÎncă nu există evaluări
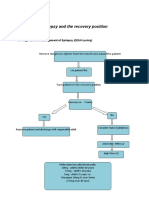
- Epilepsy Recovery Period - Second YrDocument3 paginiEpilepsy Recovery Period - Second YrBrian MaloneyÎncă nu există evaluări
- Diabetes Mellitus: Regulation of Blood GlucoseDocument65 paginiDiabetes Mellitus: Regulation of Blood GlucoseReggae BautistaÎncă nu există evaluări
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 paginiDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいÎncă nu există evaluări
- InvokanaDocument14 paginiInvokanaalvaroÎncă nu există evaluări
- Basal Bolus Insulin Titration AhsDocument2 paginiBasal Bolus Insulin Titration AhsAnn A.100% (1)
- Drug Educ Long Term Effects of AlcoholDocument7 paginiDrug Educ Long Term Effects of Alcoholmary rose ombrogÎncă nu există evaluări
- Chronic Pancreatitis: DR.E.KAUSHIK KUMAR, MS Post Graduate Stanley Medical College & HospitalDocument47 paginiChronic Pancreatitis: DR.E.KAUSHIK KUMAR, MS Post Graduate Stanley Medical College & HospitalYash SharmaÎncă nu există evaluări
- AHG-deprescribing-algorithms-2018-English AntidiabeticDocument2 paginiAHG-deprescribing-algorithms-2018-English Antidiabeticmuhammad irsyad khresna ajiÎncă nu există evaluări
- Farmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikDocument42 paginiFarmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikAnonymous h76WT2cFdkÎncă nu există evaluări
- QuotesDocument41 paginiQuotesTrishenth FonsekaÎncă nu există evaluări
- CASE ON DYSLIPIDEMIA by SriramDocument13 paginiCASE ON DYSLIPIDEMIA by SriramSriram SuryaÎncă nu există evaluări