S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Learn SpanishDocument96 paginiLearn Spanishv155r100% (64)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- From Head To Toe PDFDocument14 paginiFrom Head To Toe PDFRaquel López Juan100% (4)
- Cambridge English Speaking Sample PapersDocument6 paginiCambridge English Speaking Sample PapersGabriel LopezÎncă nu există evaluări
- Histology Tissue Preparation MicroscopyDocument4 paginiHistology Tissue Preparation MicroscopyNel TinduganiÎncă nu există evaluări
- Common Errors By Spanish Speakers Learning EnglishDocument4 paginiCommon Errors By Spanish Speakers Learning EnglishNati Rodriguez GilÎncă nu există evaluări
- Uick Tart: Start Your New Life in 15 Minutes or Less!Document44 paginiUick Tart: Start Your New Life in 15 Minutes or Less!Nati Rodriguez GilÎncă nu există evaluări
- Cambridge Science Year 7 LB Lyp Removed CompressedDocument268 paginiCambridge Science Year 7 LB Lyp Removed CompresseddivyamohandasÎncă nu există evaluări
- 7 Areas of Learning and DevelopmentDocument1 pagină7 Areas of Learning and DevelopmentNati Rodriguez GilÎncă nu există evaluări
- iMovie Movie CreationDocument14 paginiiMovie Movie CreationNati Rodriguez Gil0% (1)
- Discover Animals Behind Containers in Dear Zoo StoryDocument10 paginiDiscover Animals Behind Containers in Dear Zoo StoryNati Rodriguez Gil100% (1)
- IELTS Handbook 2007Document22 paginiIELTS Handbook 2007srikwaits4u100% (15)
- Acessorios FTIRDocument52 paginiAcessorios FTIRanagabriela12Încă nu există evaluări
- Activity Pack: Wallpaper 6 - Graphic Devices 11 Wallpaper 6 - Graphic Devices 11Document6 paginiActivity Pack: Wallpaper 6 - Graphic Devices 11 Wallpaper 6 - Graphic Devices 11Nati Rodriguez GilÎncă nu există evaluări
- PassportsDocument4 paginiPassportsNati Rodriguez GilÎncă nu există evaluări
- Tractor 2Document1 paginăTractor 2Nati Rodriguez GilÎncă nu există evaluări
- PassportDocument1 paginăPassportNati Rodriguez GilÎncă nu există evaluări
- Jingle Jingle Little BellDocument1 paginăJingle Jingle Little BellNati Rodriguez GilÎncă nu există evaluări
- 14DaysOfSuperchargedMeals PDFDocument23 pagini14DaysOfSuperchargedMeals PDFNati Rodriguez GilÎncă nu există evaluări
- 2013-Influence of Ferrule, Post System, and Length On Biomechanical Behavior of Endodontically Treated Anterior TeethDocument5 pagini2013-Influence of Ferrule, Post System, and Length On Biomechanical Behavior of Endodontically Treated Anterior TeethandreeacirsteaÎncă nu există evaluări
- Dentin AdhessionDocument23 paginiDentin AdhessionNati Rodriguez GilÎncă nu există evaluări
- Performance of Four Dentine Excavation Methods in Deciduous TeethDocument7 paginiPerformance of Four Dentine Excavation Methods in Deciduous TeethNati Rodriguez GilÎncă nu există evaluări
- IELTS Preparation and Practice: ReadingDocument15 paginiIELTS Preparation and Practice: ReadingNati Rodriguez GilÎncă nu există evaluări
- Current Challenge and Concepts of The Nickel Titanium InstrumentsDocument10 paginiCurrent Challenge and Concepts of The Nickel Titanium InstrumentsNati Rodriguez GilÎncă nu există evaluări
- The Paleo DietDocument17 paginiThe Paleo Dietgo2top283% (12)
- Crown Lengthening Via Biometric ApproachDocument8 paginiCrown Lengthening Via Biometric ApproachMohamed Ibrahem MohamedÎncă nu există evaluări
- Bacteriophage MCQsDocument3 paginiBacteriophage MCQsMahi ShafiqueÎncă nu există evaluări
- NeviDocument10 paginiNeviSafira FarihaÎncă nu există evaluări
- Cell Structure GizmoDocument5 paginiCell Structure GizmoJumana ShahataÎncă nu există evaluări
- Starrett Swiss Instruments 09 Metrology Solutions BrochureDocument16 paginiStarrett Swiss Instruments 09 Metrology Solutions BrochurecalidadcdokepÎncă nu există evaluări
- OPTIKA Microscopy Catalog - Laboratory - B-290Document16 paginiOPTIKA Microscopy Catalog - Laboratory - B-290Andrew tan chee chiatÎncă nu există evaluări
- CG Grade 7Document20 paginiCG Grade 7Maasin Sky0% (1)
- Jasco Applications Book CD and PolarimetersDocument62 paginiJasco Applications Book CD and PolarimetersDan Pantoș100% (1)
- DANAHER CORP /DE/ 10-K (Annual Reports) 2009-02-25Document332 paginiDANAHER CORP /DE/ 10-K (Annual Reports) 2009-02-25http://secwatch.comÎncă nu există evaluări
- Chapter 2 MicrobioDocument39 paginiChapter 2 MicrobioEzekiel AkameÎncă nu există evaluări
- Science 7 Q2 Week 4 LAS on Plant and Animal CellsDocument2 paginiScience 7 Q2 Week 4 LAS on Plant and Animal CellsZayn Daniel World of GamesÎncă nu există evaluări
- Group 4 Activity Sheets Answers KeyDocument6 paginiGroup 4 Activity Sheets Answers KeyClaire Angelie RuayaÎncă nu există evaluări
- 2008 Annual Report 1Document98 pagini2008 Annual Report 1Panji MittaiÎncă nu există evaluări
- Histopath-Prelim ReviewerDocument10 paginiHistopath-Prelim ReviewerKhey AgamÎncă nu există evaluări
- Iit - Bombay Annual ReportDocument96 paginiIit - Bombay Annual Reportfirefist_ashÎncă nu există evaluări
- Ultra Structure of ProkaryoteDocument3 paginiUltra Structure of ProkaryoteselvasrijaÎncă nu există evaluări
- OCR Practical Skills A Level Biology Checklist 2015Document2 paginiOCR Practical Skills A Level Biology Checklist 2015mosulÎncă nu există evaluări
- Biological Confocal Microscopy Handbook Of: Third EditionDocument28 paginiBiological Confocal Microscopy Handbook Of: Third EditionSinaid Alvarez-CervantesÎncă nu există evaluări
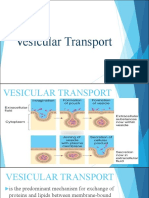
- Vesicular Transport (Group 3)Document30 paginiVesicular Transport (Group 3)Joanna RollanÎncă nu există evaluări
- Perbandingan Pengenceran Larutan Giemsa 3% Dan 5% Terhadap Pemeriksaan Morfologi PlasmodiumDocument9 paginiPerbandingan Pengenceran Larutan Giemsa 3% Dan 5% Terhadap Pemeriksaan Morfologi PlasmodiumMuti WahyuÎncă nu există evaluări
- Durham-Moore Edible Cell Project and RubricDocument2 paginiDurham-Moore Edible Cell Project and Rubricmindmover0003100% (1)
- Biological Science - Scriptwriting For SiyensikulaDocument13 paginiBiological Science - Scriptwriting For SiyensikulaJoveth TampilÎncă nu există evaluări
- Krithika Shankar Updated Resume 2023Document8 paginiKrithika Shankar Updated Resume 2023Katrina ReyesÎncă nu există evaluări
- Histology & Its Methods of StudyDocument5 paginiHistology & Its Methods of StudyByron MacalintalÎncă nu există evaluări
- Basic CytopathologyDocument10 paginiBasic CytopathologyPresheta SellappahÎncă nu există evaluări
- Light, Phase, Fluorescence Microscopes Principles & ApplicationsDocument33 paginiLight, Phase, Fluorescence Microscopes Principles & ApplicationsSomesh MahajanÎncă nu există evaluări
- Various Posters DFMDocument5 paginiVarious Posters DFMmanvik joshiÎncă nu există evaluări
- Fixed Stage Upright MicroscopeDocument14 paginiFixed Stage Upright MicroscopeAmy AdamsÎncă nu există evaluări