S-ar putea să vă placă și
- ACLS DrugDocument7 paginiACLS DrugPhongsatorn Thunin100% (1)
- ICF Model For Parkinson's DiseaseDocument8 paginiICF Model For Parkinson's Diseasehelsil01Încă nu există evaluări
- Hospital Design GuidelinesDocument33 paginiHospital Design GuidelinesRohit Gupta100% (3)
- Assessment of Clinical ReasoningDocument19 paginiAssessment of Clinical ReasoningLatha DamodaranÎncă nu există evaluări
- Clinical Localization and History in NeurologyDocument41 paginiClinical Localization and History in NeurologyRhomizal MazaliÎncă nu există evaluări
- Chapter 11 Multiple Dosage RegimenDocument35 paginiChapter 11 Multiple Dosage RegimenYuli Irvaransiah DIatun NIkmah100% (2)
- Oral Hygiene InstructionsDocument2 paginiOral Hygiene Instructionstepokpantat100% (1)
- Visual Dysfunction in Diabetes PDFDocument395 paginiVisual Dysfunction in Diabetes PDFMarcosÎncă nu există evaluări
- 4 5837051926121809399 PDFDocument119 pagini4 5837051926121809399 PDFSrinivas PingaliÎncă nu există evaluări
- PeriopConceptsDocument43 paginiPeriopConceptsKysha Huang100% (1)
- Pulmonary Tuberculosis Nclex QuestionsDocument3 paginiPulmonary Tuberculosis Nclex Questionssheen100% (6)
- Infection Prevention and Control in Linen and Laundry ManagementDocument46 paginiInfection Prevention and Control in Linen and Laundry Managementaringkinking75% (4)
- Clinical Features and Visual Outcomes of Optic Neuritis in Chinese ChildrenDocument7 paginiClinical Features and Visual Outcomes of Optic Neuritis in Chinese ChildrenklinkasikÎncă nu există evaluări
- NIH Public Access: Author ManuscriptDocument16 paginiNIH Public Access: Author ManuscriptAri Setiyawan NugrahaÎncă nu există evaluări
- BR J Ophthalmol 2005 BenEzra 444 8Document6 paginiBR J Ophthalmol 2005 BenEzra 444 8Gemilang KhusnurrokhmanÎncă nu există evaluări
- Clinical Study: Outcome and Prognostic Factors For Traumatic Endophthalmitis Over A 5-Year PeriodDocument8 paginiClinical Study: Outcome and Prognostic Factors For Traumatic Endophthalmitis Over A 5-Year PeriodannisaÎncă nu există evaluări
- Jurnal OftamologiDocument6 paginiJurnal Oftamologinurul_sharaswatiÎncă nu există evaluări
- Uveitis in Children and Adolescents: Extended ReportDocument5 paginiUveitis in Children and Adolescents: Extended ReportSelfima PratiwiÎncă nu există evaluări
- Original Research Paper OphthalmologyDocument2 paginiOriginal Research Paper OphthalmologyNurul Annisa muthaharaÎncă nu există evaluări
- Eye 2011154 ADocument7 paginiEye 2011154 AAmba PutraÎncă nu există evaluări
- Ni Hms 436399Document18 paginiNi Hms 436399Devanti EkaÎncă nu există evaluări
- 00005Document8 pagini00005drheriÎncă nu există evaluări
- JC Virus 2.0.Document9 paginiJC Virus 2.0.Kartheek VarmaÎncă nu există evaluări
- Clinical Study: Vertigo in Children and Adolescents: Characteristics and OutcomeDocument6 paginiClinical Study: Vertigo in Children and Adolescents: Characteristics and OutcomeC Leite HendriyÎncă nu există evaluări
- Behcet DiseaseDocument6 paginiBehcet DiseasejbahalkehÎncă nu există evaluări
- Mode of Presentation TBDocument7 paginiMode of Presentation TBSohaib Abbas MalikÎncă nu există evaluări
- An Examination of The Ocular Signs of Blunt Eye Injuries in A Prospective ResearchDocument4 paginiAn Examination of The Ocular Signs of Blunt Eye Injuries in A Prospective ResearchInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Classification of Visual Field Abnormalities in Highly Myopic Eyes Without Pathologic ChangeDocument26 paginiClassification of Visual Field Abnormalities in Highly Myopic Eyes Without Pathologic Change钟华Încă nu există evaluări
- Syphilitic Uveitis - EyeWikiDocument5 paginiSyphilitic Uveitis - EyeWikitgrrwccj98Încă nu există evaluări
- Characteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterDocument9 paginiCharacteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterFrancescFranquesaÎncă nu există evaluări
- Jurnal Reading GlaucomaDocument6 paginiJurnal Reading GlaucomawidyawirapÎncă nu există evaluări
- Eye Findings in Patients With Juvenile Dermatomyositis: Key Indexing TermsDocument6 paginiEye Findings in Patients With Juvenile Dermatomyositis: Key Indexing TermsOana BiancaÎncă nu există evaluări
- Glaucoma OHTSDocument13 paginiGlaucoma OHTSJose Antonio Fuentes VegaÎncă nu există evaluări
- Steriod Cataract PDFDocument4 paginiSteriod Cataract PDFLisa IskandarÎncă nu există evaluări
- Ocular Involvement and Visual Outcome of Herpes Zoster Ophthalmicus: Review of 45 Patients From Tunisia, North AfricaDocument6 paginiOcular Involvement and Visual Outcome of Herpes Zoster Ophthalmicus: Review of 45 Patients From Tunisia, North AfricaGiorgos MousterisÎncă nu există evaluări
- Ophthalmological Findings in Children With EncephalitisDocument8 paginiOphthalmological Findings in Children With EncephalitisSabila TasyakurÎncă nu există evaluări
- The Risk of Complications of Uveitis in A District Hospital CohortDocument6 paginiThe Risk of Complications of Uveitis in A District Hospital CohortSelfima PratiwiÎncă nu există evaluări
- Oct 2Document8 paginiOct 2Star LadyÎncă nu există evaluări
- Glaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandraDocument5 paginiGlaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandranjmdrÎncă nu există evaluări
- Analysis of The Clinical Diagnosis and Treatment of UveitisDocument7 paginiAnalysis of The Clinical Diagnosis and Treatment of UveitisRhysandÎncă nu există evaluări
- Changes in Contrast Sensitivity in Young Adults With DiabetesDocument5 paginiChanges in Contrast Sensitivity in Young Adults With Diabetesnurahmi widyani ratriÎncă nu există evaluări
- Epidemiology of Angioid Streaks-Associated Choroidal Neovascular Membranes in The United KingdomDocument20 paginiEpidemiology of Angioid Streaks-Associated Choroidal Neovascular Membranes in The United KingdomCureusÎncă nu există evaluări
- Correlation of Visual Field Defects and Optical Coherence Tomography Finding in Migraine PatientsDocument5 paginiCorrelation of Visual Field Defects and Optical Coherence Tomography Finding in Migraine Patientsmara 11Încă nu există evaluări
- High Myopia and Glaucoma Susceptibility The Beijing Eye StudyDocument5 paginiHigh Myopia and Glaucoma Susceptibility The Beijing Eye StudyDickyStevanoZukhriÎncă nu există evaluări
- Sicca Syndrome in Patients HIVDocument6 paginiSicca Syndrome in Patients HIVkagone walidÎncă nu există evaluări
- Hemorrhagic Unilateral RetinopathyDocument7 paginiHemorrhagic Unilateral RetinopathyHanna_RÎncă nu există evaluări
- Comparison of Visual Outcomes in Coats' Disease A 20-Year ExperienceDocument9 paginiComparison of Visual Outcomes in Coats' Disease A 20-Year ExperienceMuhammad Ihsan AuliaÎncă nu există evaluări
- Research Article 'S Disease: Severity of Ocular: Vision-Threatening Behcet Involvement PredictorsDocument7 paginiResearch Article 'S Disease: Severity of Ocular: Vision-Threatening Behcet Involvement PredictorsdeswitrigintaÎncă nu există evaluări
- Jurnal 3Document6 paginiJurnal 3Adrianus NyomanÎncă nu există evaluări
- Clinical Profile of Tubercular Uveitis in A Tertiary Care Ophthalmic CentreDocument3 paginiClinical Profile of Tubercular Uveitis in A Tertiary Care Ophthalmic CentreArif BudimanÎncă nu există evaluări
- Evaluation of The Relationship Between Binocular Anomaly and Headache Prospective Cross Sectional StudyDocument7 paginiEvaluation of The Relationship Between Binocular Anomaly and Headache Prospective Cross Sectional StudyEstefania GuerreroÎncă nu există evaluări
- VT For TBI (Ciuffreda Optomety 2010)Document5 paginiVT For TBI (Ciuffreda Optomety 2010)Synapgen ArticlesÎncă nu există evaluări
- Demographic and Clinical Profile of Patients Who Underwent Refractive Surgery ScreeningDocument8 paginiDemographic and Clinical Profile of Patients Who Underwent Refractive Surgery ScreeningPierre A. RodulfoÎncă nu există evaluări
- Medicina 59 01660 v2Document10 paginiMedicina 59 01660 v2Maria CorbuÎncă nu există evaluări
- 9 Samuel EtalDocument4 pagini9 Samuel EtaleditorijmrhsÎncă nu există evaluări
- Orbital Cellulitis in A Pediatric Population - Experience From A Tertiary CenterDocument3 paginiOrbital Cellulitis in A Pediatric Population - Experience From A Tertiary CenterMuthu V RanÎncă nu există evaluări
- Articol 14.05Document7 paginiArticol 14.05Ilina Lavinia IoanaÎncă nu există evaluări
- A Clinical Study of Anterior Uveitis in A Rural Hospital: DR - Anitha.S.Maiya, DR - Sundip ShenoyDocument5 paginiA Clinical Study of Anterior Uveitis in A Rural Hospital: DR - Anitha.S.Maiya, DR - Sundip ShenoyTri BasukiÎncă nu există evaluări
- 2016 Article 310Document6 pagini2016 Article 310Gracie ShemaÎncă nu există evaluări
- Pi Is 0161642012005052Document8 paginiPi Is 0161642012005052Pra BowoÎncă nu există evaluări
- 2014 IIHTTDesignand MethodsDocument12 pagini2014 IIHTTDesignand MethodsSIMON PEREZ LOPEZÎncă nu există evaluări
- Intracranial Tumors: An Ophthalmic Perspective: DR M Hemanandini, DR P Sumathi, DR P A KochamiDocument3 paginiIntracranial Tumors: An Ophthalmic Perspective: DR M Hemanandini, DR P Sumathi, DR P A Kochamiwolfang2001Încă nu există evaluări
- Jurnal ReadingDocument27 paginiJurnal ReadingPatresya LantanÎncă nu există evaluări
- NIH Public Access: Author ManuscriptDocument17 paginiNIH Public Access: Author ManuscriptLaura Paola UrquizoÎncă nu există evaluări
- Parinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronDocument6 paginiParinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronJessica HerreraÎncă nu există evaluări
- Presentation, Etiology, and Outcome of Brain Infections in An Indonesian HospitalDocument15 paginiPresentation, Etiology, and Outcome of Brain Infections in An Indonesian HospitalANISA RIFKA RIDHOÎncă nu există evaluări
- Journal 3Document6 paginiJournal 3riskab123Încă nu există evaluări
- Endophthalmitis Patients Seen in A Tertiary Eye Care Centre in Odisha: A Clinico-Microbiological AnalysisDocument8 paginiEndophthalmitis Patients Seen in A Tertiary Eye Care Centre in Odisha: A Clinico-Microbiological AnalysisSurendar KesavanÎncă nu există evaluări
- Controversies in Neuro-Ophthalmic Management: An Evidence and Case-Based AppraisalDe la EverandControversies in Neuro-Ophthalmic Management: An Evidence and Case-Based AppraisalAmanda D. HendersonÎncă nu există evaluări
- Posterior Uveitis: Advances in Imaging and TreatmentDe la EverandPosterior Uveitis: Advances in Imaging and TreatmentNarsing A. RaoÎncă nu există evaluări
- As Far As Possible - en ISO 14971Document19 paginiAs Far As Possible - en ISO 14971Kanwal Jit Singh100% (1)
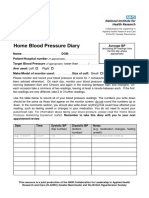
- Home Blood Pressure DiaryDocument2 paginiHome Blood Pressure DiaryCherieÎncă nu există evaluări
- Laser Retinopexy PDFDocument4 paginiLaser Retinopexy PDFveerroxxÎncă nu există evaluări
- Health Claim Form Part BDocument3 paginiHealth Claim Form Part BShubham PandeyÎncă nu există evaluări
- SclerademaDocument5 paginiSclerademaMichael SponslerÎncă nu există evaluări
- Shouldice NotesDocument3 paginiShouldice NotesDisha TutejaÎncă nu există evaluări
- Panel Hospital ListDocument4 paginiPanel Hospital ListNoman_Saeed_1520100% (1)
- Guia Tiva 2018Document14 paginiGuia Tiva 2018John Bryan Herrera DelgadoÎncă nu există evaluări
- Pre and Post Op Management of Surgical PatientsDocument36 paginiPre and Post Op Management of Surgical PatientsPrabhakar KumarÎncă nu există evaluări
- Nursing Care and Do-Not-Resuscitate (DNR) Decisions: PurposeDocument6 paginiNursing Care and Do-Not-Resuscitate (DNR) Decisions: PurposeBea-ayesha A. PandaoÎncă nu există evaluări
- Encopresis and EnuresisDocument10 paginiEncopresis and EnuresisRoci ArceÎncă nu există evaluări
- Oxygen TherapyDocument36 paginiOxygen TherapyabdihakemÎncă nu există evaluări
- Case Study PcosDocument6 paginiCase Study Pcosapi-315331895Încă nu există evaluări
- Sydney M PRPDocument23 paginiSydney M PRPapi-465406877Încă nu există evaluări
- Corneal Degenerations and DystrophiesDocument12 paginiCorneal Degenerations and DystrophiesSuleman MuhammadÎncă nu există evaluări
- Reaction PaperDocument4 paginiReaction PaperClark David Panganiban100% (1)
- Acute Limb Ischemic: Titien Buniyati Ali Aspar MappahyaDocument40 paginiAcute Limb Ischemic: Titien Buniyati Ali Aspar MappahyaNurhasanah WahabÎncă nu există evaluări
- Benign Skin TumoursDocument7 paginiBenign Skin TumoursMan LorÎncă nu există evaluări
- Naim Oral CareDocument34 paginiNaim Oral Carenaim157Încă nu există evaluări
- Syllabus Refreshing of First Aid Intermediate Level For Synthetic Rubber Indonesia Security TeamDocument5 paginiSyllabus Refreshing of First Aid Intermediate Level For Synthetic Rubber Indonesia Security TeamRobbyAjiAryaÎncă nu există evaluări