S-ar putea să vă placă și
- Maternal Mortality Remains Major Challenge To Health Systems WorldwideDocument2 paginiMaternal Mortality Remains Major Challenge To Health Systems WorldwidePety Tunjung SariÎncă nu există evaluări
- Appendicitis Medication - Penicillins, Cephalosporins, Aminoglycosides, Carbapenems, Fluoroquinolones, Anti-Infective Agents, AnalgesicsDocument5 paginiAppendicitis Medication - Penicillins, Cephalosporins, Aminoglycosides, Carbapenems, Fluoroquinolones, Anti-Infective Agents, AnalgesicsPety Tunjung SariÎncă nu există evaluări
- Appendicitis Clinical Presentation - History, Physical Examination, Appendicitis and PregnancyDocument6 paginiAppendicitis Clinical Presentation - History, Physical Examination, Appendicitis and PregnancyPety Tunjung SariÎncă nu există evaluări
- Appendicitis Differential DiagnosesDocument5 paginiAppendicitis Differential DiagnosesPety Tunjung SariÎncă nu există evaluări
- Maternal Mortality Remains Major Challenge To Health Systems WorldwideDocument2 paginiMaternal Mortality Remains Major Challenge To Health Systems WorldwidePety Tunjung SariÎncă nu există evaluări
- CandidiasisDocument6 paginiCandidiasisyorlandaÎncă nu există evaluări
- Effect of Removable Partial Denture On Periodontal HealthDocument3 paginiEffect of Removable Partial Denture On Periodontal HealthAlex KwokÎncă nu există evaluări
- Anxiety Disorders (Risk Factors)Document3 paginiAnxiety Disorders (Risk Factors)Pety Tunjung SariÎncă nu există evaluări
- Anxiety Disorders (Risk Factors)Document3 paginiAnxiety Disorders (Risk Factors)Pety Tunjung SariÎncă nu există evaluări
- Bacterial and Viral Etiology of Childhood Diarrhea in OuagadougouDocument15 paginiBacterial and Viral Etiology of Childhood Diarrhea in OuagadougouPety Tunjung SariÎncă nu există evaluări
- Treatment of InfertilityDocument12 paginiTreatment of InfertilityPety Tunjung SariÎncă nu există evaluări
- Anatomi Fisiologi Kardiovaskular 2013Document64 paginiAnatomi Fisiologi Kardiovaskular 2013Sally WirawanÎncă nu există evaluări
- What Is Cerebral PalsyDocument2 paginiWhat Is Cerebral PalsyPety Tunjung SariÎncă nu există evaluări
- Chord Dan Kunci GitarDocument19 paginiChord Dan Kunci GitarPety Tunjung SariÎncă nu există evaluări
- Oral Rehydration Salts (ORS)Document3 paginiOral Rehydration Salts (ORS)Pety Tunjung SariÎncă nu există evaluări
- P 285Document7 paginiP 285Pety Tunjung SariÎncă nu există evaluări
- Chord Dan Kunci GitarDocument19 paginiChord Dan Kunci GitarPety Tunjung SariÎncă nu există evaluări
- WHO CDD SER 85.8 pp1-60Document62 paginiWHO CDD SER 85.8 pp1-60Pety Tunjung SariÎncă nu există evaluări
- Long Distance LyricsDocument3 paginiLong Distance LyricsPety Tunjung SariÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Dialog Bahasa InggirsDocument2 paginiDialog Bahasa InggirsKeRtha NeghaRaÎncă nu există evaluări
- Report - IvatanDocument28 paginiReport - IvatanJohara Winel PerezÎncă nu există evaluări
- QuantAssay Software Manual 11-Mar-2019Document51 paginiQuantAssay Software Manual 11-Mar-2019LykasÎncă nu există evaluări
- Properties of Matter ReviewDocument8 paginiProperties of Matter Reviewapi-290100812Încă nu există evaluări
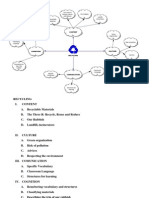
- Recycling Mind MapDocument2 paginiRecycling Mind Mapmsole124100% (1)
- PAG7.1 Student The Effects of Antibiotics On Microbial Growth - v0.3Document3 paginiPAG7.1 Student The Effects of Antibiotics On Microbial Growth - v0.3Habib UddinÎncă nu există evaluări
- 2 Contoh Narative TextDocument9 pagini2 Contoh Narative TextRini RienzÎncă nu există evaluări
- Fama Fraternitatis Rosae Crucis PDFDocument2 paginiFama Fraternitatis Rosae Crucis PDFJudy50% (2)
- Industrial Internet of Things: Presented To-Presented byDocument18 paginiIndustrial Internet of Things: Presented To-Presented byGaurav RaturiÎncă nu există evaluări
- Reactive Dyes For Digital Textile Printing InksDocument4 paginiReactive Dyes For Digital Textile Printing InksDHRUVÎncă nu există evaluări
- Abnormalities of Placenta, Amniotic Fluid and Cord: Prepared By, B. Ezhilarasi, Nursing TutorDocument21 paginiAbnormalities of Placenta, Amniotic Fluid and Cord: Prepared By, B. Ezhilarasi, Nursing TutorGopala KrishnanÎncă nu există evaluări
- Relationsh Between EM and Young S ModuliDocument7 paginiRelationsh Between EM and Young S ModuliDwight AndersonÎncă nu există evaluări
- Earth Sciences Notes Csir-Ugc Net JRFDocument57 paginiEarth Sciences Notes Csir-Ugc Net JRFmanas773Încă nu există evaluări
- Five Star Hotel and ResortDocument9 paginiFive Star Hotel and ResortAISHÎncă nu există evaluări
- Index PDFDocument159 paginiIndex PDFHüseyin IşlakÎncă nu există evaluări
- History of Flash Part - 2Document7 paginiHistory of Flash Part - 2YOGESHWER NATH SINGHÎncă nu există evaluări
- Opex and CapexDocument5 paginiOpex and CapexATM Shafiq Ul AlamÎncă nu există evaluări
- Sch3u Exam Review Ws s2018 PDFDocument4 paginiSch3u Exam Review Ws s2018 PDFwdsfÎncă nu există evaluări
- SCIENCEEEEEDocument3 paginiSCIENCEEEEEChristmae MaganteÎncă nu există evaluări
- ST 36Document4 paginiST 36ray72roÎncă nu există evaluări
- Nutrient DeficiencyDocument8 paginiNutrient Deficiencyfeiserl100% (1)
- JHS 182Document137 paginiJHS 182harbhajan singhÎncă nu există evaluări
- Aluminium Alloy - Wikipedia, The Free EncyclopediaDocument12 paginiAluminium Alloy - Wikipedia, The Free EncyclopediaAshishJoshi100% (1)
- Serial Analysis of Gene Expression (SAGE)Document34 paginiSerial Analysis of Gene Expression (SAGE)Rohit PhalakÎncă nu există evaluări
- Product Stock Exchange Learn BookDocument1 paginăProduct Stock Exchange Learn BookSujit MauryaÎncă nu există evaluări
- Chemical Bonds WorksheetDocument2 paginiChemical Bonds WorksheetJewel Mae MercadoÎncă nu există evaluări
- Reloved - October 2015Document116 paginiReloved - October 2015Barron Fields67% (3)
- TS SR Chemistry Imp Questions PDFDocument5 paginiTS SR Chemistry Imp Questions PDFUnknown Khan100% (3)
- Intro Slow Keyofg: Em7 G5 A7Sus4 G C/G D/F# AmDocument2 paginiIntro Slow Keyofg: Em7 G5 A7Sus4 G C/G D/F# Ammlefev100% (1)
- Unnatural Selection BiologyDocument2 paginiUnnatural Selection BiologyAlexa ChaviraÎncă nu există evaluări