S-ar putea să vă placă și
- PN FUNDAMENTALS: Passbooks Study GuideDe la EverandPN FUNDAMENTALS: Passbooks Study GuideÎncă nu există evaluări
- Critical Care NursingDocument85 paginiCritical Care NursinganreilegardeÎncă nu există evaluări
- INFECTION CONTROL: Passbooks Study GuideDe la EverandINFECTION CONTROL: Passbooks Study GuideÎncă nu există evaluări
- Test Bank Leading and Managing in Nursing 6th EditionDocument9 paginiTest Bank Leading and Managing in Nursing 6th EditionRichard1LauritsenÎncă nu există evaluări
- FANCAS AssessmentDocument19 paginiFANCAS AssessmentNelly Q. NisaÎncă nu există evaluări
- NR 304 SIM-CohenDocument1 paginăNR 304 SIM-CohenMORGAN CALDWELLÎncă nu există evaluări
- NR465 VSim Prep Guide & Guided ReadingDocument10 paginiNR465 VSim Prep Guide & Guided ReadingSam DanaÎncă nu există evaluări
- Chapter 26Document46 paginiChapter 26meeeenonÎncă nu există evaluări
- Final PRC Evaluation ToolDocument9 paginiFinal PRC Evaluation Toolbladimer_riaÎncă nu există evaluări
- 1 Perspectives of Pediatric NursingDocument57 pagini1 Perspectives of Pediatric NursingBluebloodboyÎncă nu există evaluări
- The Future of Nursing EducationDocument7 paginiThe Future of Nursing EducationJose Vicente A. Faderon100% (1)
- Evidence Based Nursing Practice by GridoDocument42 paginiEvidence Based Nursing Practice by GridoVivin Karlina100% (1)
- Using SBAR Communications in Efforts To Prevent.8Document12 paginiUsing SBAR Communications in Efforts To Prevent.8Sheena Cabriles100% (2)
- Deep Sternal Wound Infections: Evidence For Prevention, Treatment, and Reconstructive SurgeryDocument12 paginiDeep Sternal Wound Infections: Evidence For Prevention, Treatment, and Reconstructive Surgerylsintaningtyas100% (1)
- Pharmacology Syllabus Bio 408 Sum 2017Document6 paginiPharmacology Syllabus Bio 408 Sum 2017Grafika DiahÎncă nu există evaluări
- CEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsDocument18 paginiCEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsLauren GarciaÎncă nu există evaluări
- Chapter 2 Family Centered Community Based CareDocument2 paginiChapter 2 Family Centered Community Based CareBlake McCabeÎncă nu există evaluări
- What Is InformaticsDocument38 paginiWhat Is Informaticsapi-239123914Încă nu există evaluări
- Safety Unfolding Nursing Case StudyDocument3 paginiSafety Unfolding Nursing Case StudyclarimerÎncă nu există evaluări
- EBP Poster Template 2019Document1 paginăEBP Poster Template 2019Momina ArshadÎncă nu există evaluări
- ENA Leadership Conference 2013 ProgramDocument17 paginiENA Leadership Conference 2013 ProgramEmergency Nurses AssociationÎncă nu există evaluări
- Clinical ExemplarDocument4 paginiClinical Exemplarapi-272451466Încă nu există evaluări
- Professional Development PowerpointDocument12 paginiProfessional Development Powerpointapi-400385739Încă nu există evaluări
- Problem#1Document3 paginiProblem#1jas lacsonÎncă nu există evaluări
- Nursing Study Guide Answer KeyDocument174 paginiNursing Study Guide Answer KeyDENNIS N. MUÑOZÎncă nu există evaluări
- Nursing Handover of Vital Signs at The Transition of Care Fromthe Emergency Department To The Inpatient Ward Anintegrative ReviewDocument12 paginiNursing Handover of Vital Signs at The Transition of Care Fromthe Emergency Department To The Inpatient Ward Anintegrative ReviewLilac SpaceÎncă nu există evaluări
- Handwashing NSG Research Paper 2022Document7 paginiHandwashing NSG Research Paper 2022Kathy LaminackÎncă nu există evaluări
- NursingDocument57 paginiNursingremzylicious100% (1)
- Gero NursingDocument9 paginiGero NursingcmsaonlineÎncă nu există evaluări
- نسخة Lecture - PAIN Assessment & ManagementDocument52 paginiنسخة Lecture - PAIN Assessment & Managementjsoal100% (1)
- Spices ToolDocument2 paginiSpices ToolTrisha Fae Loyola BalagotÎncă nu există evaluări
- Dec06np5 Nursing Care of Client With PhysiologicalDocument11 paginiDec06np5 Nursing Care of Client With PhysiologicaljavadahuttÎncă nu există evaluări
- Clinical Nursing JudgementDocument5 paginiClinical Nursing Judgementapi-502199148100% (1)
- Sbar Simulation ReflectionDocument3 paginiSbar Simulation Reflectionapi-314635911100% (2)
- Final-Research Proposal Group 7Document49 paginiFinal-Research Proposal Group 7Kristalyn Mary Dimas Diwayan - AlcagnoÎncă nu există evaluări
- E NursingDocument16 paginiE Nursinggopscharan100% (1)
- Simple Guide For Basic Nursing InterventionsDocument13 paginiSimple Guide For Basic Nursing InterventionsMelvin NizelÎncă nu există evaluări
- GCOE Provision 4-6Document29 paginiGCOE Provision 4-6Justine May GervacioÎncă nu există evaluări
- Class 1 Introduction To Clinical PharmacologyDocument33 paginiClass 1 Introduction To Clinical Pharmacologymustafa 1Încă nu există evaluări
- StatementDocument5 paginiStatementtrinity_brannonÎncă nu există evaluări
- Skilled Discharge Planning FormDocument3 paginiSkilled Discharge Planning FormRini Fauzia AÎncă nu există evaluări
- Incontinence Case StudyDocument26 paginiIncontinence Case StudyRose AnnÎncă nu există evaluări
- Nursing AdministrationDocument38 paginiNursing AdministrationNinez Manzanillo-BalmadridÎncă nu există evaluări
- Shift Assessment of Nursing DocumentationDocument18 paginiShift Assessment of Nursing DocumentationQwequ Gong Ananse100% (3)
- Jarvis Chapter 18 Study GuideDocument5 paginiJarvis Chapter 18 Study GuideEmily Cheng100% (2)
- Emergency Medical TechnicianDocument2 paginiEmergency Medical Technicianapi-78482557Încă nu există evaluări
- Evolution of Nursing Theories - PowerpointDocument122 paginiEvolution of Nursing Theories - PowerpointLea Lovelle Malabanan100% (2)
- Core Competencies, 2012 NNCCSDocument23 paginiCore Competencies, 2012 NNCCSJose BernelÎncă nu există evaluări
- Diseases, Syndromes & Health Events Under SurveillanceDocument61 paginiDiseases, Syndromes & Health Events Under SurveillanceGina BoligaoÎncă nu există evaluări
- Legal Implications Document A Schneider PDFDocument52 paginiLegal Implications Document A Schneider PDFAmrod Inglorion100% (2)
- Care Planning & Reflection PresentationDocument48 paginiCare Planning & Reflection PresentationBatool Al-Shabrakha100% (1)
- Maternal+Newborn+Matrix+Packet+KEY Spr+2019+ (MR)Document6 paginiMaternal+Newborn+Matrix+Packet+KEY Spr+2019+ (MR)lisa mornoÎncă nu există evaluări
- Clinical Placement Summary 2018 Barwon Health GeelongDocument9 paginiClinical Placement Summary 2018 Barwon Health Geelongapi-569029509Încă nu există evaluări
- Care of Adults 26 Endocrine ManagementDocument26 paginiCare of Adults 26 Endocrine ManagementGaras AnnaBerniceÎncă nu există evaluări
- 1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)Document39 pagini1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)NTRisforthinkersÎncă nu există evaluări
- Usaf Nurse Corps-Information Booklet-4feb13Document39 paginiUsaf Nurse Corps-Information Booklet-4feb13Jorge Vigoreaux100% (1)
- Case StudyPainDocument1 paginăCase StudyPainlovesalad100% (1)
- Nursing Home Lesson PlanDocument13 paginiNursing Home Lesson Planapi-353466401100% (1)
- Survey Sucess With KinnserDocument12 paginiSurvey Sucess With KinnserKinnser SoftwareÎncă nu există evaluări
- Logbook TemplateDocument3 paginiLogbook TemplateJoeren GonzalesÎncă nu există evaluări
- Allergies or Food Intolerances.: Therapeutic DietDocument3 paginiAllergies or Food Intolerances.: Therapeutic DietBryan Mae H. DegorioÎncă nu există evaluări
- Introduction To Change: Towards Excellence: "PHIC Accredited Health Care Provider"Document3 paginiIntroduction To Change: Towards Excellence: "PHIC Accredited Health Care Provider"Bryan Mae H. DegorioÎncă nu există evaluări
- Drug Cal - Practice TestDocument2 paginiDrug Cal - Practice TestBryan Mae H. DegorioÎncă nu există evaluări
- Sampling Process and Measurement ScaleDocument18 paginiSampling Process and Measurement ScaleBryan Mae H. DegorioÎncă nu există evaluări
- Drugs Affecting The Immune SystemDocument4 paginiDrugs Affecting The Immune SystemBryan Mae H. DegorioÎncă nu există evaluări
- Worksheet in BloodDocument12 paginiWorksheet in BloodBryan Mae H. DegorioÎncă nu există evaluări
- Systems of Measurement and Drug CalculationDocument13 paginiSystems of Measurement and Drug CalculationBryan Mae H. DegorioÎncă nu există evaluări
- Is Mentorship For YOUDocument17 paginiIs Mentorship For YOUBryan Mae H. DegorioÎncă nu există evaluări
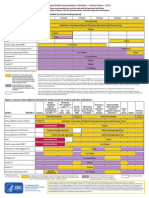
- Adult Immunization ScheduleDocument3 paginiAdult Immunization ScheduleBryan Mae H. DegorioÎncă nu există evaluări
- Skeletal SystemDocument27 paginiSkeletal SystemBryan Mae H. DegorioÎncă nu există evaluări
- NMC Standards To Support Learning AssessmentDocument85 paginiNMC Standards To Support Learning AssessmentBryan Mae H. DegorioÎncă nu există evaluări
- Care of Patient With Musculoskeletal DisordersDocument3 paginiCare of Patient With Musculoskeletal DisordersBryan Mae H. DegorioÎncă nu există evaluări
- APA Referencing 6th Ed Quick GuideDocument2 paginiAPA Referencing 6th Ed Quick GuidehartymÎncă nu există evaluări
- EmbryologyDocument26 paginiEmbryologyBryan Mae H. Degorio100% (1)
- Disaster Nursing and ManagementDocument39 paginiDisaster Nursing and ManagementBryan Mae H. DegorioÎncă nu există evaluări
- APA Referencing 6th Ed Quick GuideDocument2 paginiAPA Referencing 6th Ed Quick GuidehartymÎncă nu există evaluări
- Documentation and ReportingDocument32 paginiDocumentation and ReportingBryan Mae H. Degorio100% (1)
- The Adult LearningDocument15 paginiThe Adult LearningBryan Mae H. DegorioÎncă nu există evaluări
- Skeletal SystemDocument27 paginiSkeletal SystemBryan Mae H. DegorioÎncă nu există evaluări
- Key (10) Principles of CST - 1 PagerDocument1 paginăKey (10) Principles of CST - 1 PagerBryan Mae H. DegorioÎncă nu există evaluări
- Is Mentorship For YOUDocument17 paginiIs Mentorship For YOUBryan Mae H. DegorioÎncă nu există evaluări
- Bowel PreparationDocument2 paginiBowel PreparationBryan Mae H. DegorioÎncă nu există evaluări
- Preceptor Handbook For Nursing EducationDocument41 paginiPreceptor Handbook For Nursing EducationBryan Mae H. Degorio0% (1)
- Human Immunodeficiency Virus /AIDSDocument7 paginiHuman Immunodeficiency Virus /AIDSBryan Mae H. DegorioÎncă nu există evaluări
- Kidney Disease: Underwriter FocusDocument3 paginiKidney Disease: Underwriter FocusBryan Mae H. DegorioÎncă nu există evaluări
- Disaster Nursing and ManagementDocument39 paginiDisaster Nursing and ManagementBryan Mae H. DegorioÎncă nu există evaluări
- Concept Mapping BMDDocument4 paginiConcept Mapping BMDBryan Mae H. DegorioÎncă nu există evaluări
- 04 Tissue, Glands and MembranesDocument52 pagini04 Tissue, Glands and MembranesBryan Mae H. Degorio100% (1)
- Case Studies For Bowel EliminationDocument2 paginiCase Studies For Bowel EliminationBryan Mae H. Degorio100% (2)
- Jeep TJ Torque SpecsDocument4 paginiJeep TJ Torque SpecsmaulotaurÎncă nu există evaluări
- 实用多元统计分析Document611 pagini实用多元统计分析foo-hoat LimÎncă nu există evaluări
- Olp Lesson PlanDocument2 paginiOlp Lesson Planapi-654865620Încă nu există evaluări
- Arithmetic Mean PDFDocument29 paginiArithmetic Mean PDFDivya Gothi100% (1)
- Tabulation Sheet (LABO)Document9 paginiTabulation Sheet (LABO)KetIanCotalesÎncă nu există evaluări
- Commissioning 1. Commissioning: ES200 EasyDocument4 paginiCommissioning 1. Commissioning: ES200 EasyMamdoh EshahatÎncă nu există evaluări
- CERADocument10 paginiCERAKeren Margarette AlcantaraÎncă nu există evaluări
- 4 Qi Imbalances and 5 Elements: A New System For Diagnosis and TreatmentDocument5 pagini4 Qi Imbalances and 5 Elements: A New System For Diagnosis and Treatmentpixey55100% (1)
- Psych PresurgicalDocument31 paginiPsych Presurgicalriham ammar100% (1)
- 160 78-m1Document70 pagini160 78-m1George100% (7)
- Liebherr PR 712 Litronic Final DrivesDocument8 paginiLiebherr PR 712 Litronic Final DrivesLiebherr75% (4)
- Marketing Research Completed RevisedDocument70 paginiMarketing Research Completed RevisedJodel DagoroÎncă nu există evaluări
- Sa Inc HCP English d10840Document64 paginiSa Inc HCP English d10840Ayu AfiantyÎncă nu există evaluări
- Artikel 8 - (CURRICULUM EVALUATION)Document12 paginiArtikel 8 - (CURRICULUM EVALUATION)Kikit8Încă nu există evaluări
- Thesis Final 2 Number c1-c5Document167 paginiThesis Final 2 Number c1-c5Kimverly DomaganÎncă nu există evaluări
- Bashar CitateDocument7 paginiBashar CitateCristiana ProtopopescuÎncă nu există evaluări
- Brochure Delegation Training For LeadersDocument6 paginiBrochure Delegation Training For LeadersSupport ALProgramsÎncă nu există evaluări
- IRremote Library, Send & Receive Infrared Remote ControlDocument4 paginiIRremote Library, Send & Receive Infrared Remote ControlJayant SwamiÎncă nu există evaluări
- Exercise Chapter 4 This Is How You Do ItDocument10 paginiExercise Chapter 4 This Is How You Do ItAgustina WidiyantiÎncă nu există evaluări
- Grade 7 - R & C - Where Tigers Swim - JanDocument15 paginiGrade 7 - R & C - Where Tigers Swim - JanKritti Vivek100% (3)
- Defining The Christian Faith PaperDocument8 paginiDefining The Christian Faith Paperlin tongÎncă nu există evaluări
- TSM 101 Course Outline (2022)Document2 paginiTSM 101 Course Outline (2022)ChryseanjÎncă nu există evaluări
- D904 - D906 - D914 - D916 - D924 - D926 - 8718458 - 04092008 - v02 - enDocument218 paginiD904 - D906 - D914 - D916 - D924 - D926 - 8718458 - 04092008 - v02 - enАлексей89% (18)
- Impact of Technology On Our LivesDocument3 paginiImpact of Technology On Our LivesKim ErandioÎncă nu există evaluări
- Power Factor Improvement SystemDocument25 paginiPower Factor Improvement SystemBijoy SahaÎncă nu există evaluări
- Glorious Mysteries 1Document5 paginiGlorious Mysteries 1Vincent safariÎncă nu există evaluări
- D1 001 Prof Rudi STAR - DM in Indonesia - From Theory To The Real WorldDocument37 paginiD1 001 Prof Rudi STAR - DM in Indonesia - From Theory To The Real WorldNovietha Lia FarizymelinÎncă nu există evaluări
- Theater InstallationDocument7 paginiTheater InstallationtemamÎncă nu există evaluări
- CE 2812-Permeability Test PDFDocument3 paginiCE 2812-Permeability Test PDFShiham BadhurÎncă nu există evaluări
- Heat Cured ElastomersDocument40 paginiHeat Cured ElastomerslberrierÎncă nu există evaluări
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (170)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Încă nu există evaluări
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDe la EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisEvaluare: 5 din 5 stele5/5 (8)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (58)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (45)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (253)