S-ar putea să vă placă și
- Reporting guidelines for qualitative research interviews and focus groupsDocument9 paginiReporting guidelines for qualitative research interviews and focus groupsNurul QalbyÎncă nu există evaluări
- Strategies to Prevent Catheter-Associated Urinary Tract InfectionsDocument17 paginiStrategies to Prevent Catheter-Associated Urinary Tract InfectionsKiran SurageÎncă nu există evaluări
- The Effects of Telemental Health ServicesDocument12 paginiThe Effects of Telemental Health ServicesJason SempleÎncă nu există evaluări
- Challenges & Issues in Nursing LeadershipDocument3 paginiChallenges & Issues in Nursing LeadershipFrancis Adrian50% (2)
- Risk Factors of Quality of Life Among Tuberculosis PatientsDocument7 paginiRisk Factors of Quality of Life Among Tuberculosis PatientsIJPHSÎncă nu există evaluări
- Faktor-Faktor Yang Berhubungan Dengan Kualitas Handover Pasien Di Ruang Rawat Inap Rumah SakitDocument6 paginiFaktor-Faktor Yang Berhubungan Dengan Kualitas Handover Pasien Di Ruang Rawat Inap Rumah SakitAyu PurbaÎncă nu există evaluări
- AACN BSN Essentials PaperDocument9 paginiAACN BSN Essentials PaperSikany S EmmanÎncă nu există evaluări
- Can Nurse Attitudes Improve PerformanceDocument26 paginiCan Nurse Attitudes Improve Performancemade setiniÎncă nu există evaluări
- Seminar On PhilosophyDocument37 paginiSeminar On Philosophymalleshwari athramÎncă nu există evaluări
- Telehealth Nursing: A Position StatementDocument13 paginiTelehealth Nursing: A Position StatementSheldon WilliamsÎncă nu există evaluări
- List of Idsr Priority Diseases/Condition/Events and Reporting Frequencies (Idsr 3 Edition)Document14 paginiList of Idsr Priority Diseases/Condition/Events and Reporting Frequencies (Idsr 3 Edition)Salihu MustaphaÎncă nu există evaluări
- Group 4 Controlling - BN4BDocument54 paginiGroup 4 Controlling - BN4BGlen DaleÎncă nu există evaluări
- Policy Paper 1 1Document6 paginiPolicy Paper 1 1api-316574434Încă nu există evaluări
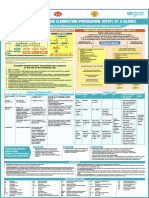
- NTEP at A Glance - Comprehensive Clinical Management Protocol For TBDocument1 paginăNTEP at A Glance - Comprehensive Clinical Management Protocol For TBNael NajeebÎncă nu există evaluări
- 3.1 ESG ReviewDocument26 pagini3.1 ESG ReviewPriyanka AggarwalÎncă nu există evaluări
- 4140 QI PosterDocument1 pagină4140 QI PosterZoe RaineÎncă nu există evaluări
- Couden - Final Chikungunya Health Impact Framework PaperDocument15 paginiCouden - Final Chikungunya Health Impact Framework Paperapi-449016836100% (1)
- 5462 - Management and Leadership in Practice - EditedDocument37 pagini5462 - Management and Leadership in Practice - Editeddouglas gacheru ngatiiaÎncă nu există evaluări
- Post Stroke DepressionDocument8 paginiPost Stroke Depressionranu anggaraÎncă nu există evaluări
- Articles Summary On Nursing ShortageDocument9 paginiArticles Summary On Nursing Shortageem0% (1)
- Differentiating Nursing Leadership and Management Competencies - ScienceDirectDocument5 paginiDifferentiating Nursing Leadership and Management Competencies - ScienceDirectAlan Divine BÎncă nu există evaluări
- Nurse Managers' Leadership Styles Impact Ward StaffDocument10 paginiNurse Managers' Leadership Styles Impact Ward StaffsintiaÎncă nu există evaluări
- Masters ThesisDocument33 paginiMasters ThesisChristine Elaine Batusin IlaganÎncă nu există evaluări
- Leadership Finnish PDFDocument17 paginiLeadership Finnish PDFpietroÎncă nu există evaluări
- Nurs501 Role Paper MSN Nursing Administrator Nicky ReedDocument9 paginiNurs501 Role Paper MSN Nursing Administrator Nicky Reedapi-215994182Încă nu există evaluări
- Nur400 NursingleadershipphilosophypaperDocument10 paginiNur400 Nursingleadershipphilosophypaperapi-489685873Încă nu există evaluări
- An Overview of 5 Year Patterns and Trends in The Journal of Nursing ManagementDocument5 paginiAn Overview of 5 Year Patterns and Trends in The Journal of Nursing ManagementMaria Gorheti DheydjawaÎncă nu există evaluări
- The Impact of Nurse Managers' Leadership Styles On Ward StaffDocument12 paginiThe Impact of Nurse Managers' Leadership Styles On Ward StaffsintiaÎncă nu există evaluări
- Sample Thesis FormatDocument35 paginiSample Thesis FormatMichael Erick Valera Virtucio100% (1)
- Nursing Leadership and ManagementDocument32 paginiNursing Leadership and ManagementWimer100% (2)
- Nursing Leadership and ManagementDocument32 paginiNursing Leadership and ManagementWimer100% (1)
- Miko LeadershipDocument6 paginiMiko LeadershipMark Anthony IbayÎncă nu există evaluări
- Nursing Leadership in An Academic Hospital in Gauteng South AfricaDocument10 paginiNursing Leadership in An Academic Hospital in Gauteng South AfricaMuhammad Fahrin AzhariÎncă nu există evaluări
- Much of The Literature Supports The Importance of An Advanced Education For The Nurse LeaderDocument9 paginiMuch of The Literature Supports The Importance of An Advanced Education For The Nurse Leaderapi-273083825Încă nu există evaluări
- Research ProposalDocument14 paginiResearch ProposalRaki' Tobias JonesÎncă nu există evaluări
- EDUCAPORDR15763Document6 paginiEDUCAPORDR15763Jackson MarwaÎncă nu există evaluări
- 2006 LeadershipDocument18 pagini2006 LeadershipcherrymaemidoriÎncă nu există evaluări
- Motivations and Barriers Among Philippine Nurses To Pursue ADocument4 paginiMotivations and Barriers Among Philippine Nurses To Pursue APaula Grace MorfeÎncă nu există evaluări
- Case Study Staff RetentionDocument28 paginiCase Study Staff Retentionjessa_guanzonÎncă nu există evaluări
- Leadership of Nurses Associated with Quality of CareDocument15 paginiLeadership of Nurses Associated with Quality of Carevan royeÎncă nu există evaluări
- Factors influencing knowledge management and nurse leaders' roleDocument14 paginiFactors influencing knowledge management and nurse leaders' roleoohscÎncă nu există evaluări
- Nursing 7.24Document5 paginiNursing 7.24murasi omamoÎncă nu există evaluări
- Nurse Manager Perspective of Staff Participation in Unit Level Shared GovernanceDocument8 paginiNurse Manager Perspective of Staff Participation in Unit Level Shared GovernanceSer Eldrin GarciaÎncă nu există evaluări
- Leadership JournalDocument2 paginiLeadership JournalRalph Elvin MacanlalayÎncă nu există evaluări
- Developing Leadership in Nursing: Exploring Core Factors: Elizabeth A. Curtis, Jan de Vries, Fintan K. SheerinDocument5 paginiDeveloping Leadership in Nursing: Exploring Core Factors: Elizabeth A. Curtis, Jan de Vries, Fintan K. SheerinfayeexeveaÎncă nu există evaluări
- Leadership Nurse 2016 IiumDocument10 paginiLeadership Nurse 2016 IiumEera ReezmaÎncă nu există evaluări
- Nurse Managers' Responsive Coaching To Facilitate Staff Nurses' Clinical Skills Development in Public Tertiary HospitalDocument10 paginiNurse Managers' Responsive Coaching To Facilitate Staff Nurses' Clinical Skills Development in Public Tertiary Hospitalvan royeÎncă nu există evaluări
- Assessment of Leadership Knowledge and Practice Among Nurse ManagersDocument12 paginiAssessment of Leadership Knowledge and Practice Among Nurse Managersheba abd elazizÎncă nu există evaluări
- Chapter 2 Literature ReviewDocument13 paginiChapter 2 Literature ReviewDamaris KambuaÎncă nu există evaluări
- Nursing Research and Practice JournalDocument10 paginiNursing Research and Practice JournalRhea RaveloÎncă nu există evaluări
- Psychological Attachment To Nursing in The Early Career: Occupational Commitment Profiles, Motivational Patterns, Retention, and PerformanceDocument19 paginiPsychological Attachment To Nursing in The Early Career: Occupational Commitment Profiles, Motivational Patterns, Retention, and PerformanceGlăvan AncaÎncă nu există evaluări
- Nursing leadership approaches from Portuguese nurses' perspectivesDocument8 paginiNursing leadership approaches from Portuguese nurses' perspectivesLyaÎncă nu există evaluări
- Nursing Theories: Foundation For Nursing Profession: I-Manager's Journal On Nursing October 2019Document7 paginiNursing Theories: Foundation For Nursing Profession: I-Manager's Journal On Nursing October 2019Joker ParkÎncă nu există evaluări
- Lamp Light On Leadership Clinical Leadership and FlorenceDocument8 paginiLamp Light On Leadership Clinical Leadership and FlorenceKriska Erika NonesaÎncă nu există evaluări
- Mendoza, M - Ms Rle ArticleDocument15 paginiMendoza, M - Ms Rle ArticleMiguel MendozaÎncă nu există evaluări
- Week 10: Essay Akper 2016Document2 paginiWeek 10: Essay Akper 2016P Ady PutraÎncă nu există evaluări
- Nursing Students Perceptions of Nursing MetaparadDocument9 paginiNursing Students Perceptions of Nursing MetaparadJustine Mae JayonaÎncă nu există evaluări
- Liderazgo en Enfermería PDFDocument20 paginiLiderazgo en Enfermería PDFLaura Camila Hernández GiraldoÎncă nu există evaluări
- Nursing PhilosophyDocument6 paginiNursing Philosophyapi-480550791Încă nu există evaluări
- Leadership and Management Name Cover PageDocument6 paginiLeadership and Management Name Cover PageWilliamKingsÎncă nu există evaluări
- Cover DepanDocument182 paginiCover DepanFebri SuryoÎncă nu există evaluări
- Instrument set for mayor surgeryDocument1 paginăInstrument set for mayor surgeryFebri SuryoÎncă nu există evaluări
- The Role of Code Blue Team'sDocument17 paginiThe Role of Code Blue Team'sFebri SuryoÎncă nu există evaluări
- 17092018Document1 pagină17092018Febri SuryoÎncă nu există evaluări
- 5 AlgorithmDocument129 pagini5 AlgorithmFebri SuryoÎncă nu există evaluări
- UMUM: (Operasi Berlangsung +/-1jam) LUMBAL: (Operasi Berlangsung +/ - 1jam)Document5 paginiUMUM: (Operasi Berlangsung +/-1jam) LUMBAL: (Operasi Berlangsung +/ - 1jam)Febri SuryoÎncă nu există evaluări
- Billing LogDocument1 paginăBilling LogRobi AmzÎncă nu există evaluări
- MFK Alkes2Document63 paginiMFK Alkes2Febri SuryoÎncă nu există evaluări
- Askep BBLRDocument3 paginiAskep BBLRFebri SuryoÎncă nu există evaluări
- Chapter 19Document1 paginăChapter 19Febri SuryoÎncă nu există evaluări
- UMUM: (Operasi Berlangsung +/-1jam) LUMBAL: (Operasi Berlangsung +/ - 1jam)Document5 paginiUMUM: (Operasi Berlangsung +/-1jam) LUMBAL: (Operasi Berlangsung +/ - 1jam)Febri SuryoÎncă nu există evaluări
- Case Processing Summary Crosstabulation Education Level BreastfeedingDocument1 paginăCase Processing Summary Crosstabulation Education Level BreastfeedingFebri SuryoÎncă nu există evaluări
- Rajiv Gandhi University of Health Sciences, Karnataka BangaloreDocument13 paginiRajiv Gandhi University of Health Sciences, Karnataka BangaloreFebri SuryoÎncă nu există evaluări
- Chapter 19Document1 paginăChapter 19Febri SuryoÎncă nu există evaluări
- Rajiv Gandhi University of Health Sciences, Karnataka BangaloreDocument13 paginiRajiv Gandhi University of Health Sciences, Karnataka BangaloreFebri SuryoÎncă nu există evaluări
- Cheat Vice SityDocument4 paginiCheat Vice SityFebri SuryoÎncă nu există evaluări
- Higher Algebra - Hall & KnightDocument593 paginiHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- HYPNOSIS AND HYPNOTHERAPY: A PRACTICAL GUIDEDocument142 paginiHYPNOSIS AND HYPNOTHERAPY: A PRACTICAL GUIDETeodora-Aurora Brebenaru100% (1)
- Terminal Performance Objective: A Detailed Lesson Plan in English For Grade 8 I. ObjectivesDocument12 paginiTerminal Performance Objective: A Detailed Lesson Plan in English For Grade 8 I. ObjectivesEdgar Gante Jr.Încă nu există evaluări
- Mix EcoprintDocument11 paginiMix EcoprintratihÎncă nu există evaluări
- Subject: Social Studies Grade: 8 Topic: Understanding Worldview MaterialsDocument10 paginiSubject: Social Studies Grade: 8 Topic: Understanding Worldview Materialsapi-390372317Încă nu există evaluări
- Benmergui Housing Policy, Slums and Sqatter Settlements in Rio de Janeiro Brazil and Buenos Aires 1948-1973 PDFDocument423 paginiBenmergui Housing Policy, Slums and Sqatter Settlements in Rio de Janeiro Brazil and Buenos Aires 1948-1973 PDFDiego RoldánÎncă nu există evaluări
- Figurative Language EssayDocument14 paginiFigurative Language EssayRosalía ImlÎncă nu există evaluări
- TridentDocument9 paginiTridentShikha GuptaÎncă nu există evaluări
- The Power of Your Subconscious Mind by D PDFDocument7 paginiThe Power of Your Subconscious Mind by D PDFRakesh MarsaleÎncă nu există evaluări
- 7 Hermetic PrinciplesDocument2 pagini7 Hermetic PrinciplesFabrizio Bertuzzi100% (2)
- 4-Tupas v. Court of AppealsDocument2 pagini4-Tupas v. Court of AppealsFelicity HuffmanÎncă nu există evaluări
- Macabenta Vs Davao Stevendor Terminal Company, GR No. L-27489Document4 paginiMacabenta Vs Davao Stevendor Terminal Company, GR No. L-27489AddAllÎncă nu există evaluări
- 165 - Shaking Hands Between Men WomenDocument9 pagini165 - Shaking Hands Between Men WomensakibpathanÎncă nu există evaluări
- Information Technology Project Management: by Jack T. MarchewkaDocument34 paginiInformation Technology Project Management: by Jack T. MarchewkaYasmitha LÎncă nu există evaluări
- RETI RUDOLPH Tonality in Modern Music PDFDocument202 paginiRETI RUDOLPH Tonality in Modern Music PDFNabernoe0% (1)
- FASB's Conceptual Framework and Social RealityDocument19 paginiFASB's Conceptual Framework and Social RealityRitesh Kumar DubeyÎncă nu există evaluări
- Trigonometry FunctionsDocument14 paginiTrigonometry FunctionsKeri-ann Millar50% (2)
- Persian 3 Minute Kobo AudiobookDocument194 paginiPersian 3 Minute Kobo AudiobookslojnotakÎncă nu există evaluări
- Beckman - 1996 - The Parsing of ProsodyDocument53 paginiBeckman - 1996 - The Parsing of ProsodyNathacia Lucena RibeiroÎncă nu există evaluări
- Drama techniques to get students talking through mimingDocument2 paginiDrama techniques to get students talking through mimingTâm TrầnÎncă nu există evaluări
- Bhabha - of Mimicry Anb Man - The Ambivalence of Colonial DiscourseDocument10 paginiBhabha - of Mimicry Anb Man - The Ambivalence of Colonial DiscourseGuerrila NowÎncă nu există evaluări
- Biodiversity Has Emerge As A Scientific Topic With A High Degree of Social Prominence and Consequently of Political ImportantDocument5 paginiBiodiversity Has Emerge As A Scientific Topic With A High Degree of Social Prominence and Consequently of Political ImportantFatin SakuraÎncă nu există evaluări
- Pythagorean Theorem Math PDFDocument2 paginiPythagorean Theorem Math PDFapi-201420601Încă nu există evaluări
- Reading Comprehension WorksheetsTerms of UseDocument25 paginiReading Comprehension WorksheetsTerms of UseSílvia Maria Vieira60% (5)
- PhilosophyDocument15 paginiPhilosophyArnab Kumar MukhopadhyayÎncă nu există evaluări
- Kohlberg Moral Stages and MoralizationDocument12 paginiKohlberg Moral Stages and MoralizationJoy Sib-aten100% (1)
- Living Water - Viktor Schauberger and The Secrets of NaturalDocument134 paginiLiving Water - Viktor Schauberger and The Secrets of NaturalGeorg P. Mueller80% (5)
- Kanarev Photon Final PDFDocument12 paginiKanarev Photon Final PDFMaiman LatoÎncă nu există evaluări
- 3rd Grade Lesson PlansDocument5 pagini3rd Grade Lesson Plansapi-3559611970% (1)
- Iim Recommendation LetterDocument2 paginiIim Recommendation LetterSuman PoudelÎncă nu există evaluări
- Effect Of Advertisement On Honda Two-Wheeler SalesDocument8 paginiEffect Of Advertisement On Honda Two-Wheeler SalesHitesh KakadiyaÎncă nu există evaluări
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (402)
- The Ultimate Guide To Memory Improvement TechniquesDe la EverandThe Ultimate Guide To Memory Improvement TechniquesEvaluare: 5 din 5 stele5/5 (34)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (13)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÎncă nu există evaluări
- The Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverDe la EverandThe Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverEvaluare: 4.5 din 5 stele4.5/5 (186)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 3.5 din 5 stele3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÎncă nu există evaluări
- Techniques Exercises And Tricks For Memory ImprovementDe la EverandTechniques Exercises And Tricks For Memory ImprovementEvaluare: 4.5 din 5 stele4.5/5 (40)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDe la EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingEvaluare: 5 din 5 stele5/5 (4)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (327)
- The Happiness Trap: How to Stop Struggling and Start LivingDe la EverandThe Happiness Trap: How to Stop Struggling and Start LivingEvaluare: 4 din 5 stele4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 5 din 5 stele5/5 (3)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDe la EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingEvaluare: 3.5 din 5 stele3.5/5 (31)
- The First Minute: How to start conversations that get resultsDe la EverandThe First Minute: How to start conversations that get resultsEvaluare: 4.5 din 5 stele4.5/5 (55)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (41)
- Secure Love: Create a Relationship That Lasts a LifetimeDe la EverandSecure Love: Create a Relationship That Lasts a LifetimeEvaluare: 5 din 5 stele5/5 (17)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDe la EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsÎncă nu există evaluări
- Summary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisDe la EverandSummary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (22)