S-ar putea să vă placă și
- Seminar 6 - Dental CementsDocument114 paginiSeminar 6 - Dental Cementsaziz2007100% (1)
- Considerations For Establishing and Maintaining Proper Occlusion in The Aesthetic Zone - Dentistry TodayDocument12 paginiConsiderations For Establishing and Maintaining Proper Occlusion in The Aesthetic Zone - Dentistry Todayaziz2007Încă nu există evaluări
- Surface Treatments of ZirconiaDocument8 paginiSurface Treatments of Zirconiaaziz2007Încă nu există evaluări
- The Platinum Foil TechniqueDocument15 paginiThe Platinum Foil Techniqueaziz2007Încă nu există evaluări
- Occlusion. Static Occlusion, Dynamic Occlusion and Guidance - Verifiable CPD Online - DentistryDocument5 paginiOcclusion. Static Occlusion, Dynamic Occlusion and Guidance - Verifiable CPD Online - Dentistryaziz2007Încă nu există evaluări
- Elective Root Canal Treatment A Review and Clinical UpdateDocument6 paginiElective Root Canal Treatment A Review and Clinical Updateaziz2007Încă nu există evaluări
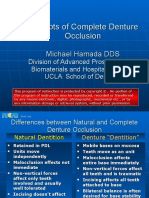
- Concepts of Complete Denture OcclusionDocument39 paginiConcepts of Complete Denture Occlusionaziz2007100% (1)
- Interdisciplinary Interface Between Fixed Prosthodontics and PeriodonticsDocument23 paginiInterdisciplinary Interface Between Fixed Prosthodontics and Periodonticsaziz20070% (1)
- Digital Impressions A New Era in ProsthodonticsDocument3 paginiDigital Impressions A New Era in Prosthodonticsaziz2007Încă nu există evaluări
- Diagnosis and Treatment Planning in FPDDocument109 paginiDiagnosis and Treatment Planning in FPDaziz2007Încă nu există evaluări
- Mandibular Movements-Bennett MovementDocument26 paginiMandibular Movements-Bennett Movementaziz2007100% (1)
- Bridge Design Part Four Bridge Design, Part Four Aesthetic Enhancement For Anterior Fixed Bridge RestorationsDocument9 paginiBridge Design Part Four Bridge Design, Part Four Aesthetic Enhancement For Anterior Fixed Bridge Restorationsaziz2007Încă nu există evaluări
- Advancements in CAD CAM TechnologyDocument13 paginiAdvancements in CAD CAM Technologyaziz2007100% (2)
- Increased Vertical Dimension of Occlusion Signs Symptoms Diagnosis Treatment and OptionsDocument6 paginiIncreased Vertical Dimension of Occlusion Signs Symptoms Diagnosis Treatment and Optionsaziz2007Încă nu există evaluări
- Re-Re-evaluation of The Condylar Path As The Reference of OcclusionDocument10 paginiRe-Re-evaluation of The Condylar Path As The Reference of Occlusionaziz2007Încă nu există evaluări
- Accuracy of Full-Arch Scans Using Intraoral ScannersDocument8 paginiAccuracy of Full-Arch Scans Using Intraoral Scannersaziz2007Încă nu există evaluări
- Perio 13-14Document164 paginiPerio 13-14priyasargunan50% (2)
- Lasers in Prosthodontics The21st CenturyDocument32 paginiLasers in Prosthodontics The21st Centuryaziz2007Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Factor Analysis of Students' Exposure To Social Media For Food and BeverageDocument6 paginiFactor Analysis of Students' Exposure To Social Media For Food and BeverageNoora ShresthaÎncă nu există evaluări
- The Union, Intersect, Minus OperatorsDocument4 paginiThe Union, Intersect, Minus Operators20f4a7bcÎncă nu există evaluări
- Article - Adolescents' Trajectories of Social Anxiety and Social WithdrawalDocument9 paginiArticle - Adolescents' Trajectories of Social Anxiety and Social WithdrawalRafael Iwamoto TosiÎncă nu există evaluări
- A Study of Covid-19 Impact On The Accademic Performance of Student in The University of Goroka by YAMSOB MOSES-Mangir 2021 DecemberDocument31 paginiA Study of Covid-19 Impact On The Accademic Performance of Student in The University of Goroka by YAMSOB MOSES-Mangir 2021 DecemberYamsob MosesÎncă nu există evaluări
- ReseachiiiiiDocument30 paginiReseachiiiiiJessie MarieÎncă nu există evaluări
- What Is The Difference Between Criteria and StandardsDocument41 paginiWhat Is The Difference Between Criteria and StandardsxredleafÎncă nu există evaluări
- Hypothesis TestDocument52 paginiHypothesis TestMusa Aman100% (1)
- Contemporary Evaluation of Teaching Challenges and PromisesDocument3 paginiContemporary Evaluation of Teaching Challenges and PromisesPaco CruzÎncă nu există evaluări
- Mba Dissertation Chapter 5Document8 paginiMba Dissertation Chapter 5BuyCheapPaperOnlineCanada100% (1)
- Introduction Course API 570Document63 paginiIntroduction Course API 570Ikade Suartana100% (1)
- B.SC StatsDocument6 paginiB.SC StatsmithunÎncă nu există evaluări
- Rubrics For Essay EvaluationDocument1 paginăRubrics For Essay EvaluationBea DeLuis de TomasÎncă nu există evaluări
- 21 198 1 PBDocument12 pagini21 198 1 PBYamburger LoveÎncă nu există evaluări
- Chapter 2 System Approach To CBM-PHMDocument22 paginiChapter 2 System Approach To CBM-PHMDioÎncă nu există evaluări
- 3.5.A AppliedStatisticsDocument4 pagini3.5.A AppliedStatisticsSophia SinghÎncă nu există evaluări
- First Written Assessment in EAPPDocument3 paginiFirst Written Assessment in EAPPRochelle AcibarÎncă nu există evaluări
- Understanding Business and Finance: Team SaralDocument18 paginiUnderstanding Business and Finance: Team Sarallakshay singlaÎncă nu există evaluări
- Chapter 3 - Research Methodology Chapter ContentsDocument31 paginiChapter 3 - Research Methodology Chapter Contentsvalentina ojeahÎncă nu există evaluări
- Intelligence AnalysisDocument36 paginiIntelligence AnalysisErik DravenÎncă nu există evaluări
- Birhanu Chane PDFDocument87 paginiBirhanu Chane PDFdawitÎncă nu există evaluări
- Exam1 PracticeDocument13 paginiExam1 PracticedrpÎncă nu există evaluări
- Tesfay Aregawi - 4Document114 paginiTesfay Aregawi - 4course heroÎncă nu există evaluări
- SynopsisDocument14 paginiSynopsisAnonymous kLc810La6100% (1)
- Bivariate AnalysisDocument19 paginiBivariate AnalysisMukteshwar Mishra100% (2)
- Welcome To Enactus: ENACTUS HANDBOOK - Meaning, Values and InterpretationDocument6 paginiWelcome To Enactus: ENACTUS HANDBOOK - Meaning, Values and InterpretationViplove SinghÎncă nu există evaluări
- Design Criteria For Steel Transmission PolesDocument25 paginiDesign Criteria For Steel Transmission PoleskunhalparikhÎncă nu există evaluări
- Skeletal Sampling and Preparation: 1.0 Principle, Spirit and IntentDocument3 paginiSkeletal Sampling and Preparation: 1.0 Principle, Spirit and IntentIsolda Alanna RlÎncă nu există evaluări
- Safety Science: Daniel PodgórskiDocument21 paginiSafety Science: Daniel PodgórskiKhovivatul IstiqomahÎncă nu există evaluări
- Stats - Lecture 1 - F2020 PDFDocument45 paginiStats - Lecture 1 - F2020 PDFHilmar Castro de GarciaÎncă nu există evaluări
- 7 HR Data Sets For People Analytics - AIHR AnalyticsDocument14 pagini7 HR Data Sets For People Analytics - AIHR AnalyticsTaha Ahmed100% (1)