S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Voice Over Script For Pilot TestingDocument2 paginiVoice Over Script For Pilot TestingRichelle Anne Tecson ApitanÎncă nu există evaluări
- Evaporative CoolingDocument68 paginiEvaporative Coolingshivas34regal100% (1)
- Philpost RRDocument6 paginiPhilpost RRGene AbotÎncă nu există evaluări
- Rate If Iodine and PropanoneDocument3 paginiRate If Iodine and Propanoneshareef1Încă nu există evaluări
- D.O. 221-A - Application Form (Renewal)Document1 paginăD.O. 221-A - Application Form (Renewal)Karl PagzÎncă nu există evaluări
- Approved College List: Select University Select College Type Select MediumDocument3 paginiApproved College List: Select University Select College Type Select MediumDinesh GadkariÎncă nu există evaluări
- Chapter 08 MGT 202 Good GovernanceDocument22 paginiChapter 08 MGT 202 Good GovernanceTHRISHIA ANN SOLIVAÎncă nu există evaluări
- Tutorial 3 MFRS8 Q PDFDocument3 paginiTutorial 3 MFRS8 Q PDFKelvin LeongÎncă nu există evaluări
- Internship Report PDFDocument71 paginiInternship Report PDFNafiz FahimÎncă nu există evaluări
- Newcastle University Dissertation FormatDocument6 paginiNewcastle University Dissertation FormatWriteMyEnglishPaperForMeSterlingHeights100% (1)
- Atoll 1400Document2 paginiAtoll 1400David M. SeoaneÎncă nu există evaluări
- Translations Telugu To English A ClassifDocument111 paginiTranslations Telugu To English A ClassifGummadi Vijaya KumarÎncă nu există evaluări
- NJEX 7300G: Pole MountedDocument130 paginiNJEX 7300G: Pole MountedJorge Luis MartinezÎncă nu există evaluări
- Science Grade 10 (Exam Prep)Document6 paginiScience Grade 10 (Exam Prep)Venice Solver100% (3)
- Teal Motor Co. Vs CFIDocument6 paginiTeal Motor Co. Vs CFIJL A H-DimaculanganÎncă nu există evaluări
- International Business ManagementDocument3 paginiInternational Business Managementkalaiselvi_velusamyÎncă nu există evaluări
- One and Half SindromeDocument4 paginiOne and Half SindromeYulia DamayantiÎncă nu există evaluări
- Master Data FileDocument58 paginiMaster Data Fileinfo.glcom5161Încă nu există evaluări
- List of Bird Sanctuaries in India (State-Wise)Document6 paginiList of Bird Sanctuaries in India (State-Wise)VISHRUTH.S. GOWDAÎncă nu există evaluări
- Studies - Number and Algebra P1Document45 paginiStudies - Number and Algebra P1nathan.kimÎncă nu există evaluări
- Deloitte - Introduction To TS&A - CloudDocument2 paginiDeloitte - Introduction To TS&A - Cloudsatyam100% (1)
- Measuring and Modeling Vertical Crosshead Vibration in Api-618 Reciprocating CompressorsDocument18 paginiMeasuring and Modeling Vertical Crosshead Vibration in Api-618 Reciprocating CompressorshmshawkiÎncă nu există evaluări
- Preblending of Raw Materia1Document26 paginiPreblending of Raw Materia1Mohammed Abdo100% (1)
- 0409 Book About Minoru Yamasaki, ReviewDocument4 pagini0409 Book About Minoru Yamasaki, RevieweviannÎncă nu există evaluări
- MBA-7002-20169108-68 MarksDocument17 paginiMBA-7002-20169108-68 MarksN GÎncă nu există evaluări
- PEA Comp Study - Estate Planning For Private Equity Fund Managers (ITaback, JWaxenberg 10 - 10)Document13 paginiPEA Comp Study - Estate Planning For Private Equity Fund Managers (ITaback, JWaxenberg 10 - 10)lbaker2009Încă nu există evaluări
- Limestone Standards PDFDocument2 paginiLimestone Standards PDFJacqueline BerueteÎncă nu există evaluări
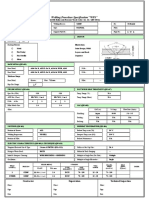
- Wps For Carbon Steel THK 7.11 GtawDocument1 paginăWps For Carbon Steel THK 7.11 GtawAli MoosaviÎncă nu există evaluări
- Reflective Memo 1-PracticumDocument5 paginiReflective Memo 1-Practicumapi-400515862Încă nu există evaluări
- Book of IQ TestsDocument124 paginiBook of IQ TestsFox Mango100% (4)