S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Acute Respiratory FailureDocument13 paginiAcute Respiratory FailureKartikaÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Critical Care Therapy and Respiratory Care Section: 1.0 DescriptionDocument7 paginiCritical Care Therapy and Respiratory Care Section: 1.0 DescriptionStefano Ignacio Valenzano FigueroaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Lecture Notes On Respiratory Medicine (Wiley, 2003) PDFDocument213 paginiLecture Notes On Respiratory Medicine (Wiley, 2003) PDFNavin ShawnÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Guide To Using Inhalers For COPD & Asthma: Smarter. Medication. ManagementDocument28 paginiA Guide To Using Inhalers For COPD & Asthma: Smarter. Medication. ManagementGUSWAN FERDIANSYAHÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Acute Exacerbation of Copd by DR Irappa MadabhaviDocument39 paginiAcute Exacerbation of Copd by DR Irappa MadabhaviIrappa MadabhaviÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
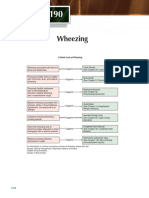
- Chapter 190: A Quick Guide to Wheezing CausesDocument1 paginăChapter 190: A Quick Guide to Wheezing CausespelinÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Effectiveness and Pharmacoeconomic Analysis of The Treatment of Severe Asthma With Omalizumab in Clinical PracticeDocument9 paginiEffectiveness and Pharmacoeconomic Analysis of The Treatment of Severe Asthma With Omalizumab in Clinical PracticePetrus Kabul TogarmaÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Test Biology 10th Class Ch#10 Gaseous ExchangeDocument1 paginăTest Biology 10th Class Ch#10 Gaseous ExchangeASAD73% (11)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Decrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromeDocument7 paginiDecrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromedarwigÎncă nu există evaluări
- 380 Case Study CDocument11 pagini380 Case Study Capi-639359658Încă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Efficacy of Retraining Diaphragm by Proprioceptive Neuromuscular Facilitation Versus Diaphragmatic Breathing Exercises in Reducing Dyspnoea in The Copd PatientsDocument4 paginiEfficacy of Retraining Diaphragm by Proprioceptive Neuromuscular Facilitation Versus Diaphragmatic Breathing Exercises in Reducing Dyspnoea in The Copd PatientsInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Announcement BIRCDocument8 paginiAnnouncement BIRCHendarsyah SuryadinataÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Respiratory Distress SyndromeDocument3 paginiRespiratory Distress SyndromeJamaica Louise Quetua MacalinoÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Weaning An Adult Patient From Invasive Mechanical VentilationDocument22 paginiWeaning An Adult Patient From Invasive Mechanical VentilationYuanda ArztÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Spirometry Interpretation: Lung VolumesDocument4 paginiSpirometry Interpretation: Lung VolumesBobet ReñaÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Asma 1Document14 paginiAsma 1Dwi Yuli YantiÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Lower Respiratory Tract InfectionDocument8 paginiLower Respiratory Tract InfectionRarasRachmandiarÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Jurnal Internasional BaruDocument4 paginiJurnal Internasional BaruCahaya YusmaniÎncă nu există evaluări
- Physical Exam For PneumoniaDocument3 paginiPhysical Exam For PneumoniaAnna SłońskaÎncă nu există evaluări
- Dupilumab COPD NEJMDocument10 paginiDupilumab COPD NEJM5fqkqkcdhtÎncă nu există evaluări
- Techniques in Cardiopulmonary PhysiotherapyDocument180 paginiTechniques in Cardiopulmonary PhysiotherapyAaliyah ShaikhÎncă nu există evaluări
- Practical Physiology RRS ResDocument9 paginiPractical Physiology RRS Resmina mounirÎncă nu există evaluări
- TuberculosisDocument475 paginiTuberculosisMaría De Los Ángeles Costta Michuy75% (4)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Bronchial AsthmaDocument59 paginiBronchial Asthmashefalika mandremÎncă nu există evaluări
- Chest and LungsDocument49 paginiChest and LungsChala KeneÎncă nu există evaluări
- Deep Breathing ExerciseDocument7 paginiDeep Breathing ExerciseRuchika Kaushal100% (5)
- Use of Expired CO Monitoring in The ICU: Dennis Bing, RRTDocument24 paginiUse of Expired CO Monitoring in The ICU: Dennis Bing, RRTasyi-2Încă nu există evaluări
- Dapus Ensefalitis 2Document4 paginiDapus Ensefalitis 2lamidahfazaÎncă nu există evaluări
- Awake Versus Deep ExtubationDocument22 paginiAwake Versus Deep Extubationtipanan_earnÎncă nu există evaluări
- G1 Health Teaching PlanDocument4 paginiG1 Health Teaching Planbernadil01Încă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)