S-ar putea să vă placă și
- Y ExercisesDocument4 paginiY ExercisesTroy Byall100% (1)
- CBB - Program Phase 1Document4 paginiCBB - Program Phase 1Titus BaldwinÎncă nu există evaluări
- Molecular and Cellular Aspects of Muscle Function: Proceedings of the 28th International Congress of Physiological Sciences Budapest 1980, (including the proceedings of the satellite symposium on Membrane Control of Skeletal Muscle Function)De la EverandMolecular and Cellular Aspects of Muscle Function: Proceedings of the 28th International Congress of Physiological Sciences Budapest 1980, (including the proceedings of the satellite symposium on Membrane Control of Skeletal Muscle Function)E. VargaÎncă nu există evaluări
- Protocol Hamstring Lengthened Eccentric Training 15214 PDFDocument9 paginiProtocol Hamstring Lengthened Eccentric Training 15214 PDFkang soon cheolÎncă nu există evaluări
- Girls and Sport: Female Athlete Triad SimplifiedDe la EverandGirls and Sport: Female Athlete Triad SimplifiedÎncă nu există evaluări
- Injury Prevention in Youth Sports.Document5 paginiInjury Prevention in Youth Sports.drmanupvÎncă nu există evaluări
- Physical Agility Test Preparation and Safety: How To Prepare For The PATDocument9 paginiPhysical Agility Test Preparation and Safety: How To Prepare For The PATJmFormalesÎncă nu există evaluări
- Landing MechanicsDocument4 paginiLanding MechanicsYunus YataganÎncă nu există evaluări
- Balance TrainingDocument12 paginiBalance TrainingMahdicheraghi100% (1)
- The 25% - 75% Rule Year-Round Training With Discipline and ToughnessDocument5 paginiThe 25% - 75% Rule Year-Round Training With Discipline and ToughnessSBD4lifeÎncă nu există evaluări
- Short Term Effects of Complex and ContrastDocument6 paginiShort Term Effects of Complex and ContrastKoordinacijska Lestev Speed LadderÎncă nu există evaluări
- Agility and Perturbation TrainingDocument19 paginiAgility and Perturbation TrainingzumantaraÎncă nu există evaluări
- Chapter 11 - RecoveryDocument20 paginiChapter 11 - RecoveryDDVÎncă nu există evaluări
- Costa Rica GlucoseDocument91 paginiCosta Rica GlucoseAnthony HarderÎncă nu există evaluări
- Optimal Shoulder Performance - Cressey ReinoldDocument40 paginiOptimal Shoulder Performance - Cressey Reinolddr_finch511Încă nu există evaluări
- Teaching The Power CleanDocument54 paginiTeaching The Power CleanStu Skalla GrimsonÎncă nu există evaluări
- 11 - Reciprocal InnervationDocument19 pagini11 - Reciprocal InnervationGaming ProÎncă nu există evaluări
- Plyometric Training Considerations To Reduce Knee.18 PDFDocument3 paginiPlyometric Training Considerations To Reduce Knee.18 PDFAndrew ShirekÎncă nu există evaluări
- Classic GPP For High School FreshmenDocument4 paginiClassic GPP For High School FreshmenxceelentÎncă nu există evaluări
- Westside Conjugate CalculatorDocument10 paginiWestside Conjugate Calculatorp300644Încă nu există evaluări
- Double Play: Training and Nutrition Advice from the World's Experts in BaseballDe la EverandDouble Play: Training and Nutrition Advice from the World's Experts in BaseballÎncă nu există evaluări
- Max Efforts Upper BodyDocument3 paginiMax Efforts Upper BodyDieter PolletÎncă nu există evaluări
- Insight From The ExpertsDocument44 paginiInsight From The Expertsjdrosenb100% (1)
- The Youth Athlete: A Practitioner’s Guide to Providing Comprehensive Sports Medicine CareDe la EverandThe Youth Athlete: A Practitioner’s Guide to Providing Comprehensive Sports Medicine CareBrian J. KrabakÎncă nu există evaluări
- PeriodizationDocument3 paginiPeriodizationAdam ZulkifliÎncă nu există evaluări
- Jumps - Plyos - Phase 1 - Upside StrengthDocument1 paginăJumps - Plyos - Phase 1 - Upside Strengthok okÎncă nu există evaluări
- Eccentric Exercise Program Design - A Periodization Model For Rehabilitation ApplicationsDocument37 paginiEccentric Exercise Program Design - A Periodization Model For Rehabilitation ApplicationsDeivison Fellipe da Silva CâmaraÎncă nu există evaluări
- Book 3: Fitness Analysis for Sport: Academy of Excellence for Coaching of Fitness DrillsDe la EverandBook 3: Fitness Analysis for Sport: Academy of Excellence for Coaching of Fitness DrillsÎncă nu există evaluări
- Chapter 12 - Injuries and Medical Care PDFDocument83 paginiChapter 12 - Injuries and Medical Care PDFDDVÎncă nu există evaluări
- Warm Ups RAMPDocument19 paginiWarm Ups RAMPRichard Jerome Dela CruzÎncă nu există evaluări
- Eccentric IsometricDocument658 paginiEccentric Isometricradarm2018555Încă nu există evaluări
- CrossFit Study (Final)Document67 paginiCrossFit Study (Final)Branimir SoljicÎncă nu există evaluări
- Justification of Training Plan-Baseball: Name: Zack Cullen Student Number: HYC50075809Document8 paginiJustification of Training Plan-Baseball: Name: Zack Cullen Student Number: HYC50075809Zack StylesÎncă nu există evaluări
- Practical Guidelines For Plyometric Intensity: PlyometricsDocument5 paginiPractical Guidelines For Plyometric Intensity: PlyometricsDDVÎncă nu există evaluări
- Dysfunctional Breathing: The Functional Screening Frequently ForgottenDocument24 paginiDysfunctional Breathing: The Functional Screening Frequently ForgottenHONGJYÎncă nu există evaluări
- Nutrition For Optimal Sports Performance: A Comprehensive GuideDocument95 paginiNutrition For Optimal Sports Performance: A Comprehensive Guidedsandos2001Încă nu există evaluări
- Core StiffnessMcGill 2015Document12 paginiCore StiffnessMcGill 2015Hugo TintiÎncă nu există evaluări
- VBT Annual Plan Dave BallouDocument8 paginiVBT Annual Plan Dave BallouEthan AtchleyÎncă nu există evaluări
- Effects of Linear and Daily UndulatingDocument20 paginiEffects of Linear and Daily UndulatingNATHALIA MARIA TORRES DA SILVAÎncă nu există evaluări
- The Effects of Eccentric Versus Concentric Resistance Training On Muscle Strength and Mass in Healthy Adults: A Systematic Review With Meta-AnalysisDocument14 paginiThe Effects of Eccentric Versus Concentric Resistance Training On Muscle Strength and Mass in Healthy Adults: A Systematic Review With Meta-AnalysisPerico PalotesÎncă nu există evaluări
- FUNHAB®: A Science-Based, Multimodal Approach For Musculoskeletal ConditionsDocument9 paginiFUNHAB®: A Science-Based, Multimodal Approach For Musculoskeletal ConditionsVizaÎncă nu există evaluări
- 2022 12 30 Website PDFDocument80 pagini2022 12 30 Website PDFmostafakhafagy8Încă nu există evaluări
- Modified Daily Undulating Periodization PDFDocument8 paginiModified Daily Undulating Periodization PDFluigiÎncă nu există evaluări
- Max Sheet Break Down Final 2 Test Back SquatDocument3 paginiMax Sheet Break Down Final 2 Test Back SquatRichard Marcus SeigelÎncă nu există evaluări
- Westside TemplateDocument3 paginiWestside TemplateSteven Yeti Griffiths100% (1)
- Love Your Bones: The essential guiding to ending osteoporosis and building a healthy skeletonDe la EverandLove Your Bones: The essential guiding to ending osteoporosis and building a healthy skeletonÎncă nu există evaluări
- Golf Performance ManualDocument35 paginiGolf Performance ManualHemang PanditÎncă nu există evaluări
- Eccentric or Concentric Exercises For The Treatment of TendinopathiesDocument11 paginiEccentric or Concentric Exercises For The Treatment of TendinopathiesAnonymous xvlg4m5xLXÎncă nu există evaluări
- Tri-Phasic Epigenetic Model of Self-AcceptanceDocument1 paginăTri-Phasic Epigenetic Model of Self-AcceptanceLucÎncă nu există evaluări
- How To Read A Training ProgramDocument13 paginiHow To Read A Training ProgramjapÎncă nu există evaluări
- Lower Extremity Stretching ProtocolDocument3 paginiLower Extremity Stretching ProtocolHello RainbowÎncă nu există evaluări
- Chapter 14 - Long Term Athletic Development in GymnasticsDocument12 paginiChapter 14 - Long Term Athletic Development in GymnasticsDDVÎncă nu există evaluări
- Boyle Phase 2 NHLDocument1 paginăBoyle Phase 2 NHLgamatttaÎncă nu există evaluări
- Functional Movement Screen and Y-Balance Test: Validity in Hamstring Injury Risk Prediction?Document74 paginiFunctional Movement Screen and Y-Balance Test: Validity in Hamstring Injury Risk Prediction?NICOLÁS ANDRÉS AYELEF PARRAGUEZÎncă nu există evaluări
- Basketball Strength & Conditioning: General PreparationDocument4 paginiBasketball Strength & Conditioning: General PreparationBaba HansÎncă nu există evaluări
- Personal Training ExercisesDocument4 paginiPersonal Training Exercisesapi-377252439Încă nu există evaluări
- Crossover Scaling Shoulder Guide 1Document6 paginiCrossover Scaling Shoulder Guide 1Alexandru SeciuÎncă nu există evaluări
- Workout ProgramDocument5 paginiWorkout Programhanus.milannseznam.czÎncă nu există evaluări
- Chapter 9 - Cardio and ESD PDFDocument28 paginiChapter 9 - Cardio and ESD PDFDDVÎncă nu există evaluări
- Performance Center Fueled By: Womens's Basketball Off-Season Level II StrengthDocument12 paginiPerformance Center Fueled By: Womens's Basketball Off-Season Level II Strengththeshow31Încă nu există evaluări
- FMSP1 PDFDocument126 paginiFMSP1 PDFPikaboo31100% (1)
- Jeremy Lewis Shoulder T and P 22nd EdDocument3 paginiJeremy Lewis Shoulder T and P 22nd EdDr Abdallah BahaaÎncă nu există evaluări
- Applied Anatomy of The ShoulderDocument11 paginiApplied Anatomy of The ShoulderSamantha HohÎncă nu există evaluări
- Final ManuscriptDocument43 paginiFinal Manuscriptapi-372150835Încă nu există evaluări
- Diseases and Disorders of The Skeletal SystemDocument32 paginiDiseases and Disorders of The Skeletal SystemPatrisha Georgia AmitenÎncă nu există evaluări
- Adhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyDocument6 paginiAdhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyRuben FigueroaÎncă nu există evaluări
- Schwerla 2020Document8 paginiSchwerla 2020João Paulo Vila Nova GomesÎncă nu există evaluări
- Shoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFDocument31 paginiShoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFElliya RosyidaÎncă nu există evaluări
- Outsmart Pain E-BookDocument69 paginiOutsmart Pain E-BookMed AliÎncă nu există evaluări
- Evidence Based Nursing Stroke 1Document6 paginiEvidence Based Nursing Stroke 1Connie SianiparÎncă nu există evaluări
- Fascial Distortion Model - Vol.4Document76 paginiFascial Distortion Model - Vol.4Magno FilhoÎncă nu există evaluări
- Effect of Taping As A Component of Conservative Treatment For Subacromial Impingement SyndromeDocument5 paginiEffect of Taping As A Component of Conservative Treatment For Subacromial Impingement SyndromeMohamed KassimÎncă nu există evaluări
- All Pages v3Document142 paginiAll Pages v3luh martaniÎncă nu există evaluări
- Rheumatology: - Syrian - Notes - CK - 2 - Step - Usmle - Pieces/8806 - Bits - CK - 2 - Step - Student - HTMLDocument5 paginiRheumatology: - Syrian - Notes - CK - 2 - Step - Usmle - Pieces/8806 - Bits - CK - 2 - Step - Student - HTMLLoyla RoseÎncă nu există evaluări
- Rotator Cuff Shoulder Pain DiagnosticDocument14 paginiRotator Cuff Shoulder Pain DiagnosticTomBramboÎncă nu există evaluări
- MKSAP Questions: Intern ReportDocument37 paginiMKSAP Questions: Intern Reportfidelurtecho4881Încă nu există evaluări
- Ultrasound-Guided Shoulder Injections in The Treatment of Subacromial BursitisDocument34 paginiUltrasound-Guided Shoulder Injections in The Treatment of Subacromial Bursitisneo079Încă nu există evaluări
- 107 Rotator Cuff Exercises - Zach CalhoonDocument136 pagini107 Rotator Cuff Exercises - Zach CalhoonSam Gregory100% (2)
- Assignment Shoulder JointDocument7 paginiAssignment Shoulder JointMary Grace OrozcoÎncă nu există evaluări
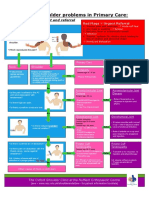
- NHS UK Diagnosis of Shoulder ProblemsDocument1 paginăNHS UK Diagnosis of Shoulder ProblemsmertÎncă nu există evaluări
- LabralDocument5 paginiLabralcrisanto ValdezÎncă nu există evaluări
- 10 2519@jospt 2020 0501 PDFDocument1 pagină10 2519@jospt 2020 0501 PDFArnold BarraÎncă nu există evaluări
- 4 - Orthopedic HistoryDocument7 pagini4 - Orthopedic HistoryshaifÎncă nu există evaluări
- Prevention of Shoulder Injuries in Overhead AthletesDocument9 paginiPrevention of Shoulder Injuries in Overhead AthletesLeonardiniÎncă nu există evaluări
- Cools 2008 Screening The Athletes Shoulder ForDocument9 paginiCools 2008 Screening The Athletes Shoulder ForLucyFloresÎncă nu există evaluări
- Biceps Tendinitis Caused by An Osteochondroma In.37Document4 paginiBiceps Tendinitis Caused by An Osteochondroma In.37harshini prakashÎncă nu există evaluări
- Sindrome Do Nervo SupraescapularDocument9 paginiSindrome Do Nervo SupraescapularAna CarolineÎncă nu există evaluări
- POMR 復健科Document6 paginiPOMR 復健科屏頂大Încă nu există evaluări
- The Effect of Scapular Protraction On Isometric Shoulder Rotation Strength in Normal SubjectsDocument5 paginiThe Effect of Scapular Protraction On Isometric Shoulder Rotation Strength in Normal SubjectskinemasÎncă nu există evaluări
- Top 3 Rotator Cuff Exercises (Fix Your Shoulder Pain)Document23 paginiTop 3 Rotator Cuff Exercises (Fix Your Shoulder Pain)Nicolas AlonsoÎncă nu există evaluări