S-ar putea să vă placă și
- Metabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentDe la EverandMetabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentCarole IchaiÎncă nu există evaluări
- Lec. 3 - Fluid and ElectrolyteDocument16 paginiLec. 3 - Fluid and Electrolyteمجيب سلطانÎncă nu există evaluări
- 3.14 Chapter 3 Water and Electrolytes Balance and ImblanceDocument140 pagini3.14 Chapter 3 Water and Electrolytes Balance and ImblanceShourav SarkarÎncă nu există evaluări
- Basic of Fluid Therapy ImaDocument69 paginiBasic of Fluid Therapy Imal Made ArtawanÎncă nu există evaluări
- Body FluidsDocument59 paginiBody FluidsAmmar SmadiÎncă nu există evaluări
- Regulation of Fluid and Electrolyte BalanceDocument43 paginiRegulation of Fluid and Electrolyte BalanceMsKizzyÎncă nu există evaluări
- Fluid Electrolyte and AcidBase BalanceDocument33 paginiFluid Electrolyte and AcidBase Balancemoncalshareen3Încă nu există evaluări
- Mabes Fluid and ElectrolytesDocument9 paginiMabes Fluid and ElectrolytesMabesÎncă nu există evaluări
- Kompartemen Cairan TubuhDocument27 paginiKompartemen Cairan Tubuhdalang leriÎncă nu există evaluări
- Water and Sodium 2024 PDFDocument61 paginiWater and Sodium 2024 PDFMpho MosehlaÎncă nu există evaluări
- Water and Electrolyte Balance: DR PreetiDocument116 paginiWater and Electrolyte Balance: DR PreetiSrishti GoenkaÎncă nu există evaluări
- Body Fluid: Presented BY DR (MRS) Okorie PDocument56 paginiBody Fluid: Presented BY DR (MRS) Okorie PKELECHI ELEJEÎncă nu există evaluări
- CH 25 of GuytonDocument7 paginiCH 25 of GuytonBea Samonte100% (2)
- Fluid and Electrolytes1Document7 paginiFluid and Electrolytes1Charl PabillonÎncă nu există evaluări
- Fluid, Electrolyte, Acid Base BalanceDocument42 paginiFluid, Electrolyte, Acid Base BalanceSutrisno YangÎncă nu există evaluări
- Fluids and ElectrolytesDocument9 paginiFluids and ElectrolytesaclumutÎncă nu există evaluări
- Lec 4Document32 paginiLec 4bosco kiuriaÎncă nu există evaluări
- S.No Table of Content Page NoDocument20 paginiS.No Table of Content Page NoTamilArasiÎncă nu există evaluări
- Fluids and Electrolytes Pathophysiology NursingDocument16 paginiFluids and Electrolytes Pathophysiology Nursinggrad_nurse_2015100% (3)
- Fluid N Electrolytes Balance - NDocument15 paginiFluid N Electrolytes Balance - NChandan SahÎncă nu există evaluări
- Fluid & Electrolyte Balance: Part 4: Regulation & MaintenanceDocument40 paginiFluid & Electrolyte Balance: Part 4: Regulation & MaintenanceMy MusicÎncă nu există evaluări
- 2012-Fluid and ElectrolytesDocument192 pagini2012-Fluid and Electrolyteskyuss2Încă nu există evaluări
- Total Body WaterDocument70 paginiTotal Body WaterZaara RashéidÎncă nu există evaluări
- Fluid and Electrolyte Balance: Presenter: Dr. Siyum Mathewos (Omfs-Ri) Modulator: Dr. Dereje (Omfs, Consultant)Document87 paginiFluid and Electrolyte Balance: Presenter: Dr. Siyum Mathewos (Omfs-Ri) Modulator: Dr. Dereje (Omfs, Consultant)Siyum MathewosÎncă nu există evaluări
- Fluids and Electrolytes FinalDocument50 paginiFluids and Electrolytes FinalOsego MokopotsaÎncă nu există evaluări
- Fluid & Electrolyte Imbalances FinalDocument142 paginiFluid & Electrolyte Imbalances FinalPriyanka T100% (3)
- 2022 Lecture 4 Body Fluids Compartments Na K 1 3Document49 pagini2022 Lecture 4 Body Fluids Compartments Na K 1 3Mariam ShenoudaÎncă nu există evaluări
- Liquidos y Electrolitos 2016Document5 paginiLiquidos y Electrolitos 2016MARIA JOSE MEDINA JAIMESÎncă nu există evaluări
- Body FluidDocument10 paginiBody FluidNwaoha Chibuzor AnthonyÎncă nu există evaluări
- F and 1Document51 paginiF and 1api-19641337Încă nu există evaluări
- Fluid and Electrolyte Imbalance PDFDocument21 paginiFluid and Electrolyte Imbalance PDFShafaq AlamÎncă nu există evaluări
- Fluid & ElectrolytesDocument85 paginiFluid & ElectrolytesAdarshBijapurÎncă nu există evaluări
- 1.1a Fluid Management 6th Seminar GRP AaDocument40 pagini1.1a Fluid Management 6th Seminar GRP AahalearnÎncă nu există evaluări
- Body Fluid 1Document55 paginiBody Fluid 1Anonymous z3afjyy1aÎncă nu există evaluări
- Fluid, Electrolyte, and Acid-Base BalanceDocument41 paginiFluid, Electrolyte, and Acid-Base BalanceRn nadeenÎncă nu există evaluări
- Body Fluida and Electrolytes PDFDocument31 paginiBody Fluida and Electrolytes PDFBeulah DasariÎncă nu există evaluări
- Fluid, Electrolyte, and Acid-Base BalanceDocument29 paginiFluid, Electrolyte, and Acid-Base BalancemeriiÎncă nu există evaluări
- Water and Electrolyte ImbalanceDocument17 paginiWater and Electrolyte Imbalancemhairat6043100% (1)
- Medical-Surgical Nursing 1Document28 paginiMedical-Surgical Nursing 1Maui Ting100% (1)
- F and e Imb .... Edu ..Document20 paginiF and e Imb .... Edu ..esakkiammalÎncă nu există evaluări
- Water LoseDocument29 paginiWater LoseJAKLIN EMPOLÎncă nu există evaluări
- Fluid and Electrolytes Lecture NotesDocument85 paginiFluid and Electrolytes Lecture NotesVince Peliño De MesaÎncă nu există evaluări
- 1a Introduction To SurgeryDocument109 pagini1a Introduction To SurgeryZllison Mae Teodoro MangabatÎncă nu există evaluări
- 02 - Body Fluids 2021Document33 pagini02 - Body Fluids 2021shabnam sajidaÎncă nu există evaluări
- 2012-Fluid and ElectrolytesDocument192 pagini2012-Fluid and ElectrolytesHarley Justiniani Dela CruzÎncă nu există evaluări
- Body Fluid, MML, 2021Document51 paginiBody Fluid, MML, 2021Boon AimanÎncă nu există evaluări
- WaterDocument16 paginiWaterAUBREY LISAYENÎncă nu există evaluări
- Body Fluids Hbc202-Lecture Notes-1Document9 paginiBody Fluids Hbc202-Lecture Notes-1Shreya AnandÎncă nu există evaluări
- Keseimbangan Cairan TubuhDocument60 paginiKeseimbangan Cairan TubuhoktavianyÎncă nu există evaluări
- 13) Body FluidsDocument20 pagini13) Body FluidsyohdeforemostÎncă nu există evaluări
- Fluid Volume BalanceDocument73 paginiFluid Volume BalanceSalman HabeebÎncă nu există evaluări
- Body FluidDocument15 paginiBody FluidrjÎncă nu există evaluări
- Body Fluids (Eng)Document27 paginiBody Fluids (Eng)Desmy FadillahÎncă nu există evaluări
- Fluids and ElectrolytesDocument7 paginiFluids and ElectrolytessetanpikulanÎncă nu există evaluări
- Fluid, Electrolyte, and Acid-Base Balance: Prepared by Janice Meeking, Mount Royal CollegeDocument96 paginiFluid, Electrolyte, and Acid-Base Balance: Prepared by Janice Meeking, Mount Royal CollegeRajesh KumarÎncă nu există evaluări
- Fluids and Electrolytes NCM 101Document142 paginiFluids and Electrolytes NCM 101France John Evangelista Torres100% (2)
- Fluid BalanceDocument50 paginiFluid Balancesiti sarahdeazÎncă nu există evaluări
- BODY Weight 100%: Balance/Imbalances & TherapyDocument11 paginiBODY Weight 100%: Balance/Imbalances & TherapyVictoria Castillo TamayoÎncă nu există evaluări
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDe la EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsÎncă nu există evaluări
- Engineering Project ListDocument25 paginiEngineering Project ListSyed ShaÎncă nu există evaluări
- Those With MoonDocument1 paginăThose With MoonRosee AldamaÎncă nu există evaluări
- Money Tree International Finance Corp. Checklist of Standard Loan RequirementsDocument2 paginiMoney Tree International Finance Corp. Checklist of Standard Loan RequirementsAgape LabuntogÎncă nu există evaluări
- Paper Specific Instructions:: GATE Chemical Engineering MSQ Paper - 1Document11 paginiPaper Specific Instructions:: GATE Chemical Engineering MSQ Paper - 1Mayank ShelarÎncă nu există evaluări
- Adenoid HypertrophyDocument56 paginiAdenoid HypertrophyWidi Yuli HariantoÎncă nu există evaluări
- Business Plan Example - Little LearnerDocument26 paginiBusiness Plan Example - Little LearnerCourtney mcintosh100% (1)
- 41 Assignment Worksheets For SchoolDocument26 pagini41 Assignment Worksheets For Schoolsoinarana456Încă nu există evaluări
- Offender TypologiesDocument8 paginiOffender TypologiesSahil AnsariÎncă nu există evaluări
- Laboratory Cold ChainDocument22 paginiLaboratory Cold ChainEmiÎncă nu există evaluări
- Starkville Dispatch Eedition 9-10-20Document12 paginiStarkville Dispatch Eedition 9-10-20The DispatchÎncă nu există evaluări
- Inlet Manifold Pressure - Test: Testing and AdjustingDocument2 paginiInlet Manifold Pressure - Test: Testing and AdjustingAbdoulaye Boua BERTHEÎncă nu există evaluări
- Kyocera Fleet Services White Paper: SecurityDocument20 paginiKyocera Fleet Services White Paper: SecurityHoratiu OanaÎncă nu există evaluări
- SPA - MichaelDocument1 paginăSPA - Michaelgilberthufana446877Încă nu există evaluări
- Recruitement Process - Siemens - Sneha Waman Kadam S200030047 PDFDocument7 paginiRecruitement Process - Siemens - Sneha Waman Kadam S200030047 PDFSneha KadamÎncă nu există evaluări
- API 510 Practise Question Nov 07 Rev1Document200 paginiAPI 510 Practise Question Nov 07 Rev1TRAN THONG SINH100% (3)
- DOWSIL™ 2-9034 Emulsion: Features & BenefitsDocument5 paginiDOWSIL™ 2-9034 Emulsion: Features & BenefitsLaban KantorÎncă nu există evaluări
- Conference Version of SB 1Document486 paginiConference Version of SB 1Paul MastersÎncă nu există evaluări
- Dungeon World ConversionDocument5 paginiDungeon World ConversionJosephLouisNadeauÎncă nu există evaluări
- Organogram - Qa / QC: Srinivasan SrinivasanDocument4 paginiOrganogram - Qa / QC: Srinivasan SrinivasanGowtham VenkatÎncă nu există evaluări
- Keratoconjunctivitis Sicca FinalDocument91 paginiKeratoconjunctivitis Sicca FinalJanki GajjarÎncă nu există evaluări
- Chapter Three Liquid Piping SystemDocument51 paginiChapter Three Liquid Piping SystemMelaku TamiratÎncă nu există evaluări
- Indian Standard (First Revision) : Method of Chemical Analysis of Hydraulic CementDocument44 paginiIndian Standard (First Revision) : Method of Chemical Analysis of Hydraulic CementArijit dasguptaÎncă nu există evaluări
- Jun Judging ClinicDocument1 paginăJun Judging Cliniccsponseller27Încă nu există evaluări
- ATI Respiratory PowerpointDocument90 paginiATI Respiratory PowerpointAnn KelseaÎncă nu există evaluări
- Care of Clients With Problems in OxygenationDocument5 paginiCare of Clients With Problems in OxygenationSkyla FiestaÎncă nu există evaluări
- Castle 1-3K E ManualDocument26 paginiCastle 1-3K E ManualShami MudunkotuwaÎncă nu există evaluări
- Lab Manual PDFDocument68 paginiLab Manual PDFSantino AwetÎncă nu există evaluări
- Chewable: Buy Pepcid AC Packages, Get Pepcid AC 18'sDocument2 paginiChewable: Buy Pepcid AC Packages, Get Pepcid AC 18'sMahemoud MoustafaÎncă nu există evaluări
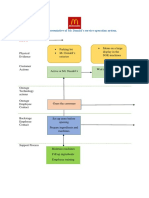
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 paginiBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênÎncă nu există evaluări
- Mil STD 792fDocument13 paginiMil STD 792fdoradoanÎncă nu există evaluări