S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Dsadertg54r 524ewegretf SDF342: SubtitleDocument11 paginiDsadertg54r 524ewegretf SDF342: SubtitleZlate TeodorÎncă nu există evaluări
- Titledasdas LayoutDocument11 paginiTitledasdas LayoutZlate TeodorÎncă nu există evaluări
- X Rayfilmreadingforbonetumour 170823234853Document81 paginiX Rayfilmreadingforbonetumour 170823234853Zlate TeodorÎncă nu există evaluări
- DsdasgreDocument11 paginiDsdasgreZlate TeodorÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Understanding Substance Abuse in AdolescentsDocument24 paginiUnderstanding Substance Abuse in AdolescentsJacqueline MansillaÎncă nu există evaluări
- HMOLEDocument12 paginiHMOLEHermie Joy MaglaquiÎncă nu există evaluări
- SDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionDocument5 paginiSDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionYwagar YwagarÎncă nu există evaluări
- 2017 Soal UAS - M. Operasional. - Bpk. Agustinus S PDFDocument3 pagini2017 Soal UAS - M. Operasional. - Bpk. Agustinus S PDFraymunandarÎncă nu există evaluări
- Test Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginDocument34 paginiTest Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginpudgyoverburnnggÎncă nu există evaluări
- Hypertension and Herbal Plant For Its Treatment: A ReviewDocument1 paginăHypertension and Herbal Plant For Its Treatment: A Reviewdyan ayu puspariniÎncă nu există evaluări
- Skilled Birth Attendant PostersDocument16 paginiSkilled Birth Attendant PostersPrabir Kumar Chatterjee100% (1)
- Dr. Miswar Fattah, M.Si. Kesiapan ATLM Dalam Melakukan Swab Nasofaring Dan Orofaring Dalam Percepatan Diagnostik COVID-19. PDSPatKLIn 18072020Document41 paginiDr. Miswar Fattah, M.Si. Kesiapan ATLM Dalam Melakukan Swab Nasofaring Dan Orofaring Dalam Percepatan Diagnostik COVID-19. PDSPatKLIn 18072020Rini WidyantariÎncă nu există evaluări
- Intro RmaDocument3 paginiIntro RmaKennery RamosÎncă nu există evaluări
- Postpartum Depression Theory (译)Document5 paginiPostpartum Depression Theory (译)彭钰莹Încă nu există evaluări
- NEWBORN CAREPLAN - VEST - FISTULA SurgicalDocument16 paginiNEWBORN CAREPLAN - VEST - FISTULA SurgicalArchana SahuÎncă nu există evaluări
- Student Medical Waiver Form: Janna Nicole CarbonelDocument1 paginăStudent Medical Waiver Form: Janna Nicole Carboneljimcarbonel05Încă nu există evaluări
- Infiltration, A New Therapy For Masking Enamel White Spot PDFDocument12 paginiInfiltration, A New Therapy For Masking Enamel White Spot PDFwijayanti siswantoÎncă nu există evaluări
- Median Rhomboid GlossitisDocument4 paginiMedian Rhomboid GlossitisYeltserÎncă nu există evaluări
- Hypertension in Pregnancy PDFDocument397 paginiHypertension in Pregnancy PDFMary PrietoÎncă nu există evaluări
- Post Mortem Technique Handbook 3HAXAPDocument465 paginiPost Mortem Technique Handbook 3HAXAPulfiani100% (2)
- For The Best Sinus Congestion RemediesDocument4 paginiFor The Best Sinus Congestion Remedies4zaleakuÎncă nu există evaluări
- Records and ReportDocument4 paginiRecords and ReportAnusikta PandaÎncă nu există evaluări
- Cleft Lip and PalateDocument25 paginiCleft Lip and PalateRahul Dhaker100% (1)
- MedicalCertificate ExmpleDocument1 paginăMedicalCertificate ExmpleJareena SamsonÎncă nu există evaluări
- Independent Nurse PractitionerDocument21 paginiIndependent Nurse PractitionerJisha Janardhan100% (1)
- PE Hyperventilation TopicDocument2 paginiPE Hyperventilation TopicJimmy Jr ChapapÎncă nu există evaluări
- Mortal Oscillatory Rates - Kook ScienceDocument20 paginiMortal Oscillatory Rates - Kook ScienceCarl MacCordÎncă nu există evaluări
- Adhd BookletDocument28 paginiAdhd BookletKitty G K'nkoÎncă nu există evaluări
- Fetal Doppler Assessment in PregnancyDocument40 paginiFetal Doppler Assessment in PregnancyKEN KIZITOÎncă nu există evaluări
- Daftar Pustaka 7689Document20 paginiDaftar Pustaka 7689Rivani KurniawanÎncă nu există evaluări
- Abstrak - Modern DressingDocument1 paginăAbstrak - Modern DressingDeny RakhmanÎncă nu există evaluări
- Denpasar Festival 2021Document4 paginiDenpasar Festival 2021Ery CorniawatiÎncă nu există evaluări
- Sepsis 3Document38 paginiSepsis 3EvanÎncă nu există evaluări
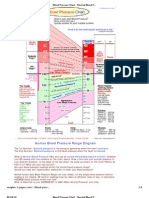
- Blood Pressure ChartDocument4 paginiBlood Pressure ChartPixelateÎncă nu există evaluări