S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- 1608 Demystifying IntelligenceDocument36 pagini1608 Demystifying IntelligenceNikolaTÎncă nu există evaluări
- Intel AcademiaDocument6 paginiIntel AcademiaNikolaTÎncă nu există evaluări
- Network Vulnerabilities ArticleDocument18 paginiNetwork Vulnerabilities ArticleNikolaTÎncă nu există evaluări
- Wetzling 1Document19 paginiWetzling 1NikolaTÎncă nu există evaluări
- Asia - Security ReviewDocument61 paginiAsia - Security ReviewNikolaTÎncă nu există evaluări
- India Web CoverDocument174 paginiIndia Web CoverNikolaTÎncă nu există evaluări
- Not Just Ideology India's Greatest Internal Security Threat Naxalites CliffordDocument13 paginiNot Just Ideology India's Greatest Internal Security Threat Naxalites CliffordNationalConferenceÎncă nu există evaluări
- Sundar-Afterword Subalterns and Sovereigns-AnAnthropologicalHistoryBastarDocument30 paginiSundar-Afterword Subalterns and Sovereigns-AnAnthropologicalHistoryBastarNikolaTÎncă nu există evaluări
- China3 0Document144 paginiChina3 0rguyÎncă nu există evaluări
- Uneasy Alliances PDFDocument12 paginiUneasy Alliances PDFNikolaTÎncă nu există evaluări
- Sundar-Afterword Subalterns and Sovereigns-AnAnthropologicalHistoryBastarDocument30 paginiSundar-Afterword Subalterns and Sovereigns-AnAnthropologicalHistoryBastarNikolaTÎncă nu există evaluări
- Guide To The Analysis of InsurgencyDocument40 paginiGuide To The Analysis of InsurgencyNikolaT100% (1)
- PunterDocument59 paginiPunterNikolaTÎncă nu există evaluări
- Left Wing Extremism in India:: Context, Implications and Response OptionsDocument44 paginiLeft Wing Extremism in India:: Context, Implications and Response OptionsNikolaTÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- 00 Worksheets 3 - Units 1-5-1Document55 pagini00 Worksheets 3 - Units 1-5-1EfrenÎncă nu există evaluări
- History of The Figure in ArtDocument48 paginiHistory of The Figure in Artcrazyleo74Încă nu există evaluări
- Qasida MuhammadiyyaDocument2 paginiQasida MuhammadiyyaFarah100% (2)
- Sell - Al-Khulafa Al-Rashidun (Four Rightly Guided Caliphs)Document38 paginiSell - Al-Khulafa Al-Rashidun (Four Rightly Guided Caliphs)Christine CareyÎncă nu există evaluări
- O Level Islamiat NotesDocument12 paginiO Level Islamiat NotesSyed Khayyam Shah101100% (3)
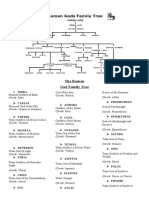
- The Roman God Family Tree: Terra Primeval Goddess of Earth (Greek: Gaia)Document2 paginiThe Roman God Family Tree: Terra Primeval Goddess of Earth (Greek: Gaia)marimar de jesusÎncă nu există evaluări
- It Is Often Said That Love Conquers AllDocument3 paginiIt Is Often Said That Love Conquers AllLilibeth100% (1)
- VergilDocument9 paginiVergilRoxana Innuendini LegezynskaÎncă nu există evaluări
- Ester Bianchi The Tantric Rebirth Movement in Modern ChinaDocument24 paginiEster Bianchi The Tantric Rebirth Movement in Modern Chinanew_libero2896Încă nu există evaluări
- Greek Orthodox Archdiocese of AmericaDocument13 paginiGreek Orthodox Archdiocese of AmericatechzonesÎncă nu există evaluări
- Visitors To The Inner Earth VDocument163 paginiVisitors To The Inner Earth VfrançoisÎncă nu există evaluări
- Calculating Arudha LagnaDocument3 paginiCalculating Arudha Lagnarahul106Încă nu există evaluări
- Koerner, Envisioning Effective Ministry. Evangelism in A Muslim ContextDocument3 paginiKoerner, Envisioning Effective Ministry. Evangelism in A Muslim ContextRezart BekaÎncă nu există evaluări
- RBL Chron 2 Page SyncDocument2 paginiRBL Chron 2 Page Synckarekare10Încă nu există evaluări
- LAT Past Paper 5 September 2020Document14 paginiLAT Past Paper 5 September 2020leomuhammadusmanÎncă nu există evaluări
- Blissful Chant: Chanting The Bliss Mantra or PurashcharanamDocument2 paginiBlissful Chant: Chanting The Bliss Mantra or PurashcharanamJithendra KumarÎncă nu există evaluări
- Martin Luther King JR - Letter From Birmingham Jail ExcerptDocument2 paginiMartin Luther King JR - Letter From Birmingham Jail ExcerptgottsackerÎncă nu există evaluări
- Contract Law OutlineDocument13 paginiContract Law Outlinesomeguy8133100% (1)
- Eastern Perspectives On Positive PsychologyDocument21 paginiEastern Perspectives On Positive PsychologyAyushi Shakya67% (6)
- KLP 9 - Jurnal Antropologi-1Document14 paginiKLP 9 - Jurnal Antropologi-1Tiara MutiaÎncă nu există evaluări
- Activity 2.1 - Film Reflection PaperDocument2 paginiActivity 2.1 - Film Reflection PaperHoward G. SumayangÎncă nu există evaluări
- Eco FeminismDocument14 paginiEco FeminismTushar KhannaÎncă nu există evaluări
- Dao Yin (導引) Training: 1. Postural Dao Yin 2. Respiratory Dao Yin Mental Dao YinDocument1 paginăDao Yin (導引) Training: 1. Postural Dao Yin 2. Respiratory Dao Yin Mental Dao YinWan Sek ChoonÎncă nu există evaluări
- MacbethperseveranceessayDocument6 paginiMacbethperseveranceessayapi-352342733Încă nu există evaluări
- Summary For Ruth Chronicles DillardDocument3 paginiSummary For Ruth Chronicles DillardJesse Amiel Aspacio-Ruiz RamosoÎncă nu există evaluări
- New International Reader's Version (NIrV) Translation EndorsementsDocument1 paginăNew International Reader's Version (NIrV) Translation EndorsementsZondervanÎncă nu există evaluări
- The Spiritual Benefits of FastingDocument2 paginiThe Spiritual Benefits of Fastingvvan1980Încă nu există evaluări
- Teaching Basic Chinese - My Own HandoutsDocument32 paginiTeaching Basic Chinese - My Own Handouts3telnik100% (1)
- Bixler v. Scientology: Declaration of Cedric Bixler-ZavalaDocument4 paginiBixler v. Scientology: Declaration of Cedric Bixler-ZavalaTony OrtegaÎncă nu există evaluări
- Ganesha Statue - Handcrafted, Divine Idol For Home Decor and Spiritual SpacesDocument16 paginiGanesha Statue - Handcrafted, Divine Idol For Home Decor and Spiritual SpacesExoticindianartÎncă nu există evaluări