S-ar putea să vă placă și
- Laboratory Monitoring When Prescribing PsychotropicsDocument5 paginiLaboratory Monitoring When Prescribing PsychotropicswaleskacrzÎncă nu există evaluări
- Medication Conversion ChartDocument2 paginiMedication Conversion ChartIlinca mirnoviciÎncă nu există evaluări
- Psychotherapist'S Guide To Psychopharmacology: Second EditionDe la EverandPsychotherapist'S Guide To Psychopharmacology: Second EditionEvaluare: 5 din 5 stele5/5 (6)
- Commonly Prescribed Psychotropic MedicationsDocument2 paginiCommonly Prescribed Psychotropic MedicationsDragutin PetrićÎncă nu există evaluări
- Pharmacology - (5) Psychotic DrugsDocument8 paginiPharmacology - (5) Psychotic DrugsSamantha DiegoÎncă nu există evaluări
- Antidepressant Therapy Algorithm PDFDocument12 paginiAntidepressant Therapy Algorithm PDFiwul kiwul KriwulÎncă nu există evaluări
- Psych DrugsDocument3 paginiPsych DrugsSwarna BanikÎncă nu există evaluări
- Medication Fact Book for Psychiatric Practice, Fifth EditionDe la EverandMedication Fact Book for Psychiatric Practice, Fifth EditionÎncă nu există evaluări
- Psychotropic Medication ReviewDocument7 paginiPsychotropic Medication ReviewAakash Shah100% (1)
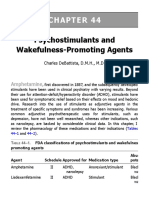
- New Developments in The Management of NarcolepsyDocument19 paginiNew Developments in The Management of Narcolepsypeppers226647dndsh34Încă nu există evaluări
- Translate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeDocument76 paginiTranslate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeHadi GunaÎncă nu există evaluări
- 2 - Diagnosis & Classification in PsychiatryDocument22 pagini2 - Diagnosis & Classification in PsychiatryKholoud KholoudÎncă nu există evaluări
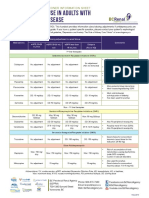
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 paginăAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Handbook of Psychiatry 2021 v2 Sample 1Document73 paginiHandbook of Psychiatry 2021 v2 Sample 1Dragutin PetrićÎncă nu există evaluări
- Psychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDocument80 paginiPsychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDennis RagudoÎncă nu există evaluări
- Unit 9 - Mental HealthDocument35 paginiUnit 9 - Mental HealthKhushi GillÎncă nu există evaluări
- Pharmacotherapy in PschiatryDocument8 paginiPharmacotherapy in PschiatryygfhdgÎncă nu există evaluări
- Practical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryDocument29 paginiPractical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryShahinaz ShamsÎncă nu există evaluări
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 paginiAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonÎncă nu există evaluări
- GP/Locum Drug List - 5 May 2013: RespiratoryDocument14 paginiGP/Locum Drug List - 5 May 2013: RespiratoryAdam ChungÎncă nu există evaluări
- Specific Drug Olanzapine (Classification IndicationDocument14 paginiSpecific Drug Olanzapine (Classification IndicationRIZZA JANE VELASCOÎncă nu există evaluări
- The RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathDocument2 paginiThe RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathRahul RaiÎncă nu există evaluări
- 504 - Pediatric Psychopharmacology - General PrinciplesDocument54 pagini504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroÎncă nu există evaluări
- Mental Health and Psychiatric Nursing: Vernalin B. Terrado, RNDocument35 paginiMental Health and Psychiatric Nursing: Vernalin B. Terrado, RNverna100% (1)
- Drugs For NeurolepticsDocument1 paginăDrugs For Neurolepticssyamil_daudÎncă nu există evaluări
- Psychotropic Drugs.Document15 paginiPsychotropic Drugs.Xiaoqing SongÎncă nu există evaluări
- Introduction To NeuropharmacologyDocument6 paginiIntroduction To Neuropharmacologyammarhafez78100% (1)
- DOPAMINE SYN, TRAN, DEGR and ReceptorsDocument15 paginiDOPAMINE SYN, TRAN, DEGR and ReceptorsRaghuram MiryalaÎncă nu există evaluări
- Obat-Obat Psychiatry - 1 2018Document104 paginiObat-Obat Psychiatry - 1 2018Christo LimbongÎncă nu există evaluări
- Adhd Toolkit MedicationsDocument1 paginăAdhd Toolkit MedicationsreneezÎncă nu există evaluări
- Mental Status Exam Template 03Document1 paginăMental Status Exam Template 03رجمه ديوان100% (1)
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 paginiShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenÎncă nu există evaluări
- DSM-IV Criteria MnemonicsDocument4 paginiDSM-IV Criteria Mnemonicsleonyap100% (1)
- Psychiatric Work-Up Template For StudentsDocument2 paginiPsychiatric Work-Up Template For StudentsTommy FuÎncă nu există evaluări
- Diabetes Mellitus Drug ChartDocument3 paginiDiabetes Mellitus Drug Chartlui.stephanie1751100% (1)
- Antipsychotics Guidelines PDFDocument31 paginiAntipsychotics Guidelines PDFZulvikar Umasangadji100% (1)
- Psychopharmacology Basics and Beyond Tolisano 2019Document109 paginiPsychopharmacology Basics and Beyond Tolisano 2019Anil Kumar100% (1)
- Pharmacology in PsychiatryDocument33 paginiPharmacology in PsychiatryKatrina PonceÎncă nu există evaluări
- What Is SchizophreniaDocument19 paginiWhat Is SchizophreniaSheena Arnoco ToraynoÎncă nu există evaluări
- Benzodiazepine Equivalents DassaDocument2 paginiBenzodiazepine Equivalents DassaPsikiater PanturaÎncă nu există evaluări
- Treatment Modalities For Mood DisordersDocument55 paginiTreatment Modalities For Mood DisordersGlory MimiÎncă nu există evaluări
- Psychopharmacology in PsychiatryDocument94 paginiPsychopharmacology in PsychiatryOslo SaputraÎncă nu există evaluări
- Common Psychiatric TermsDocument6 paginiCommon Psychiatric TermsKatrina Heart Rauto AvilaÎncă nu există evaluări
- Drug List Psych Optho NeuroDocument22 paginiDrug List Psych Optho NeuroAshley BarrileÎncă nu există evaluări
- Antidepressants and AntipsychoticsDocument50 paginiAntidepressants and AntipsychoticsPintu Bhushan MitraÎncă nu există evaluări
- AntidepressantsDocument5 paginiAntidepressantsUm HamoOd100% (2)
- AntipsychoticsDocument10 paginiAntipsychoticswawing16Încă nu există evaluări
- B /G C U I R: Anti-PsychoticsDocument2 paginiB /G C U I R: Anti-PsychoticsErsy Sakti ilhamÎncă nu există evaluări
- Review of Antipsychotic DrugsDocument15 paginiReview of Antipsychotic DrugsTuanthonBoonlue100% (1)
- Pharmacology 402 February 24, 2010 Mark Hamblin, MD, PHDDocument54 paginiPharmacology 402 February 24, 2010 Mark Hamblin, MD, PHDKarmila Novianti100% (1)
- Schizophrenia ReportDocument6 paginiSchizophrenia ReportAnna Reeka AmadorÎncă nu există evaluări
- Second and Third Generation Antipsychotics: A Comprehensive HandbookDe la EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookEvaluare: 5 din 5 stele5/5 (1)
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocument72 paginiCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116Încă nu există evaluări
- Drugs ReviewDocument230 paginiDrugs ReviewRey Mark GedaroÎncă nu există evaluări
- Psychotropic DrugsDocument49 paginiPsychotropic DrugsHanya Bint PotawanÎncă nu există evaluări
- PsychopharmacologyDocument148 paginiPsychopharmacologyAsther Mantua100% (2)
- Anidepressant Drugs: Pratik KhanalDocument37 paginiAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Antipsychotic DrugsDocument47 paginiAntipsychotic DrugsIkram UddinÎncă nu există evaluări
- Overview of Psychotropic DrugsDocument7 paginiOverview of Psychotropic Drugsnad101Încă nu există evaluări
- Side Effects of Anti Psychotic MedicationsDocument11 paginiSide Effects of Anti Psychotic MedicationsluciapopÎncă nu există evaluări
- Daftar Obat Praktek DR - Mardiana: Analgetik &anti PiretikDocument8 paginiDaftar Obat Praktek DR - Mardiana: Analgetik &anti Piretikklinik dr NandoÎncă nu există evaluări
- Neurological Pharmacology PresentationDocument49 paginiNeurological Pharmacology PresentationAmit MartinÎncă nu există evaluări
- Chapter 1 Introduction To Biopharmaceutics and Pharmacokinetics 1Document92 paginiChapter 1 Introduction To Biopharmaceutics and Pharmacokinetics 1Marc Alamo100% (2)
- Schatzberg5th-Textbook of Psychopharmacology. (1) - 1692-1698Document7 paginiSchatzberg5th-Textbook of Psychopharmacology. (1) - 1692-1698Natalia MartínezÎncă nu există evaluări
- Antidepressant AgentsDocument38 paginiAntidepressant AgentsdidiÎncă nu există evaluări
- Medications For FibromyalgiaDocument3 paginiMedications For FibromyalgiaAl ClarkeÎncă nu există evaluări
- Discrepancies in ApprovalsDocument13 paginiDiscrepancies in ApprovalsHari ThekkethilÎncă nu există evaluări
- Books and RateDocument48 paginiBooks and RateSubbiahRamasamyÎncă nu există evaluări
- Garuda 5s Ecologies of PotencyDocument20 paginiGaruda 5s Ecologies of PotencyLama GyurmeÎncă nu există evaluări
- Agomelatina WC500046224 PDFDocument3 paginiAgomelatina WC500046224 PDFElena MartinÎncă nu există evaluări
- NODocument5 paginiNODemang SatrioÎncă nu există evaluări
- FurosemideDocument1 paginăFurosemideCassie100% (1)
- Laxative Guidelines Nov 2013Document2 paginiLaxative Guidelines Nov 2013Purim KTshipÎncă nu există evaluări
- Price List Medicines Action Medeor Tanzania 05 2018Document6 paginiPrice List Medicines Action Medeor Tanzania 05 2018ABILAH SALUMÎncă nu există evaluări
- Pharmacist's Knowledge, Practice and Attitudes Toward Pharmacovigilance and Adverse Drug Reactions Reporting ProcessDocument7 paginiPharmacist's Knowledge, Practice and Attitudes Toward Pharmacovigilance and Adverse Drug Reactions Reporting ProcessAnnafiatu zakiahÎncă nu există evaluări
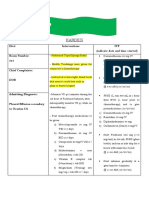
- Kardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313Document2 paginiKardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313kuro hanabusaÎncă nu există evaluări
- Introduction To Dosage FormDocument3 paginiIntroduction To Dosage FormMyPharmapediaÎncă nu există evaluări
- Pharm D SyllabusDocument120 paginiPharm D SyllabusDR Salih Ibrahim60% (5)
- Vista India: Fixed Revised Price-List Month of July-2018Document6 paginiVista India: Fixed Revised Price-List Month of July-2018malay987Încă nu există evaluări
- Application of Limulus Amebocyte Lysate (Lal) Test For Detecting Endotoxin (Pyrogen) in Large Volume ParenteralsDocument6 paginiApplication of Limulus Amebocyte Lysate (Lal) Test For Detecting Endotoxin (Pyrogen) in Large Volume ParenteralsOula HatahetÎncă nu există evaluări
- Betahistine (DRUG LIST)Document2 paginiBetahistine (DRUG LIST)Bon- BonÎncă nu există evaluări
- Application To Expedite Registration: Regulatory Authority (DRA), BhutanDocument7 paginiApplication To Expedite Registration: Regulatory Authority (DRA), BhutanSonam TsheringÎncă nu există evaluări
- OptalginDocument2 paginiOptalginanon_813207394Încă nu există evaluări
- The Importance of An Accurate and Honest Observership Program EvaluationDocument12 paginiThe Importance of An Accurate and Honest Observership Program EvaluationMaria DoukaÎncă nu există evaluări
- Formulation and Evaluation of Floating Matrix Tablets of TelmisartanDocument11 paginiFormulation and Evaluation of Floating Matrix Tablets of TelmisartanPharma Research LibraryÎncă nu există evaluări
- Cara Efektif Melakukan Stock OpnameDocument126 paginiCara Efektif Melakukan Stock OpnameDita PrimandariÎncă nu există evaluări
- Data Obat HormonDocument74 paginiData Obat HormonWizzyAsklepiosÎncă nu există evaluări
- Remifentanil Pharmacology PDFDocument41 paginiRemifentanil Pharmacology PDFamin138irÎncă nu există evaluări
- Censo Discapacitados CPT II Ruta 20iiDocument8 paginiCenso Discapacitados CPT II Ruta 20iikarlais salasÎncă nu există evaluări
- Ominous Octet For PharmacistsDocument16 paginiOminous Octet For PharmaciststreeshadowÎncă nu există evaluări