S-ar putea să vă placă și
- Antibiotic Decision Making in IcuDocument11 paginiAntibiotic Decision Making in IcumalvindersahiÎncă nu există evaluări
- Congestive Heart Failure and Pulmonary Edema Concept MapDocument1 paginăCongestive Heart Failure and Pulmonary Edema Concept MapAndrew Godwin100% (5)
- Clinical Log Term II PDFDocument9 paginiClinical Log Term II PDFPriscilla S100% (1)
- Acute Kidney FailureDocument8 paginiAcute Kidney FailureRaidis PangilinanÎncă nu există evaluări
- Pharmacokinetics & Pharmacodynamics PDFDocument31 paginiPharmacokinetics & Pharmacodynamics PDFhuong LÎncă nu există evaluări
- Gastrointestinal Bleeding, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandGastrointestinal Bleeding, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- AsthmaDocument46 paginiAsthmaHafiz Muhammad AeymonÎncă nu există evaluări
- DiverticulitisDocument2 paginiDiverticulitisyapyapvinx50% (2)
- Bloodborne PathogensDocument19 paginiBloodborne PathogensSergeiÎncă nu există evaluări
- CellulitisDocument12 paginiCellulitisAlma Bertos-Agub100% (1)
- Non-St Segment Elevation Myocardial Infarction (Nstemi)Document24 paginiNon-St Segment Elevation Myocardial Infarction (Nstemi)MHIEMHOIÎncă nu există evaluări
- Diabetes Mellitus - Diabetic KetoacidosisDocument21 paginiDiabetes Mellitus - Diabetic KetoacidosisJamil Lorca100% (5)
- Qatar Airways Cabin Crew RequirementsDocument3 paginiQatar Airways Cabin Crew RequirementsSergei75% (4)
- Qatar Airways Cabin Crew RequirementsDocument3 paginiQatar Airways Cabin Crew RequirementsSergei75% (4)
- Case Presentation OsteomylitisDocument64 paginiCase Presentation OsteomylitisDemi Rose Bolivar100% (1)
- Concept Map SepsisDocument4 paginiConcept Map SepsisSavanna ChambersÎncă nu există evaluări
- SbarDocument2 paginiSbarbojums100% (2)
- Pathophysiology of NephrosclerosisDocument2 paginiPathophysiology of NephrosclerosisJessica Damasen Caballero0% (1)
- Myocardial InfarctionDocument28 paginiMyocardial Infarctionshaitabligan100% (1)
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 paginiNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel0% (1)
- Diabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)Document5 paginiDiabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)MrRightÎncă nu există evaluări
- Concept Map On CVA Bleed Left Thalamo-Ganglionic Bleed Patient Name: Mr. DGDDocument1 paginăConcept Map On CVA Bleed Left Thalamo-Ganglionic Bleed Patient Name: Mr. DGDBert Brian Bolido100% (1)
- Pathophysiology in Liver CirrhosisDocument4 paginiPathophysiology in Liver CirrhosisCyrus Ortalla RobinÎncă nu există evaluări
- Braden Q Scale PDFDocument1 paginăBraden Q Scale PDFSri NiningÎncă nu există evaluări
- Individualized Teaching Plan Brief Patient Description/backgroundDocument2 paginiIndividualized Teaching Plan Brief Patient Description/backgroundNicole LichtenbergÎncă nu există evaluări
- Gordon's 11 Functional Health Patterns AssessmentDocument2 paginiGordon's 11 Functional Health Patterns Assessmentmtuckrn84% (37)
- Classic Radiology SignsDocument9 paginiClassic Radiology SignsJui DirDapÎncă nu există evaluări
- Case Study HyperkalemiaDocument10 paginiCase Study HyperkalemiaJamaica Cerrero100% (1)
- Nursing Care Plan For Heart Failure ChronicDocument26 paginiNursing Care Plan For Heart Failure ChronicbrantÎncă nu există evaluări
- HyperkalemiaDocument3 paginiHyperkalemiaSergeiÎncă nu există evaluări
- Gastrectomy Post OpDocument5 paginiGastrectomy Post Opfeirri100% (4)
- Abdominal Aortic AneurysmDocument14 paginiAbdominal Aortic AneurysmjialinÎncă nu există evaluări
- TCA Suppression and DM1Document22 paginiTCA Suppression and DM1Rubyrose TagumÎncă nu există evaluări
- Biodatas 601-700Document17 paginiBiodatas 601-700Nishant ChandraÎncă nu există evaluări
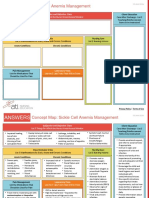
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 paginiNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- Metabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandMetabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Nursing Care Plan Renal FailureDocument18 paginiNursing Care Plan Renal FailureKundan KumarÎncă nu există evaluări
- CHF Concept MapDocument4 paginiCHF Concept MapLisaSanders99Încă nu există evaluări
- Intracranial HemorrhageDocument41 paginiIntracranial Hemorrhagedoctormussieaberra100% (1)
- COLCHICINE pptx1800128929Document15 paginiCOLCHICINE pptx1800128929April Mergelle LapuzÎncă nu există evaluări
- Decreased Cardiac Output RM 7Document9 paginiDecreased Cardiac Output RM 7api-283470660Încă nu există evaluări
- Ineffective Cerebral Tissue Perfusion Related ToDocument7 paginiIneffective Cerebral Tissue Perfusion Related TohannahÎncă nu există evaluări
- Electrolyte Imbalance 1Document3 paginiElectrolyte Imbalance 1Marius Clifford BilledoÎncă nu există evaluări
- Concept Map (Aplastic Anemia) b1Document6 paginiConcept Map (Aplastic Anemia) b1Ran PioloÎncă nu există evaluări
- Week 10 Drug Card - Hydrochlorothiazide (HCTZ)Document2 paginiWeek 10 Drug Card - Hydrochlorothiazide (HCTZ)RCurry09Încă nu există evaluări
- Nursing Care Plan Impaired Gas ExchangeDocument1 paginăNursing Care Plan Impaired Gas ExchangeKarylle PetilÎncă nu există evaluări
- Case Study 2Document7 paginiCase Study 2desdav100% (1)
- Acute Kidney Injury Concept MapDocument1 paginăAcute Kidney Injury Concept MapKEn PilapilÎncă nu există evaluări
- Lacunar Stroke Guide - Causes, Symptoms and Treatment OptionsDocument6 paginiLacunar Stroke Guide - Causes, Symptoms and Treatment OptionsRismanto TorsioÎncă nu există evaluări
- Careplan For Sickle Cell DiseaseDocument21 paginiCareplan For Sickle Cell DiseaseEcaroh Hew SmailliwÎncă nu există evaluări
- Omeprazole DSDocument2 paginiOmeprazole DSjenniferducaoÎncă nu există evaluări
- Nursing Care Plan HF FinalDocument10 paginiNursing Care Plan HF FinalCristina L. JaysonÎncă nu există evaluări
- Nursing 215 Care Plan 2 FinalDocument7 paginiNursing 215 Care Plan 2 Finalapi-283303129Încă nu există evaluări
- HypokalemiaDocument7 paginiHypokalemiaNader SmadiÎncă nu există evaluări
- NCPDocument9 paginiNCPKarell Eunice Estrellado Gutierrez100% (1)
- Congestive Heart Failure 1 Concept Map !Document1 paginăCongestive Heart Failure 1 Concept Map !Franklin A. Salaum IIIÎncă nu există evaluări
- Care Plan For Excess Fluid Volume ExampleDocument3 paginiCare Plan For Excess Fluid Volume ExampleVette Angelikka Dela CruzÎncă nu există evaluări
- IBSDocument1 paginăIBSIris MambuayÎncă nu există evaluări
- SIADH (Syndrome of Inapproperiate Antidiuretic Hormone Secretion)Document11 paginiSIADH (Syndrome of Inapproperiate Antidiuretic Hormone Secretion)itsmesubu100% (2)
- Lewis Heart Failure Care PlanDocument4 paginiLewis Heart Failure Care Plansarahbearcoups100% (1)
- Angina Pectoris PathophysiologyDocument2 paginiAngina Pectoris PathophysiologyALIANA KIMBERLY MALQUESTOÎncă nu există evaluări
- NCP and DStudyDocument8 paginiNCP and DStudyJessica Rosan Hewald ManapatÎncă nu există evaluări
- Management of HypokalemiaDocument6 paginiManagement of HypokalemiaEsraa Abu elelaÎncă nu există evaluări
- Urinary Tract Infection, (UTI) Is An Infection of One orDocument4 paginiUrinary Tract Infection, (UTI) Is An Infection of One orLorebellÎncă nu există evaluări
- Drug StudyDocument44 paginiDrug StudyLohrhen Lheighh CahreeniyowÎncă nu există evaluări
- Respiratory AcidosisDocument5 paginiRespiratory Acidosisapi-376421583% (6)
- Nursing Care PlanDocument22 paginiNursing Care PlanjamÎncă nu există evaluări
- Final Major Case StudyDocument17 paginiFinal Major Case Studyapi-546876878Încă nu există evaluări
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDe la EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideÎncă nu există evaluări
- Skills For Care Presentation Web Version Standard 1Document19 paginiSkills For Care Presentation Web Version Standard 1SergeiÎncă nu există evaluări
- HypovolemiaDocument2 paginiHypovolemiaSergeiÎncă nu există evaluări
- Nihongo NarauDocument13 paginiNihongo NarauSergeiÎncă nu există evaluări
- Diabetes SlideshowDocument17 paginiDiabetes SlideshowSergeiÎncă nu există evaluări
- Book 1Document50 paginiBook 1SergeiÎncă nu există evaluări
- SEQOHS CertificateDocument2 paginiSEQOHS CertificateSergeiÎncă nu există evaluări
- HPEX 358-002 - Basics of EpidemiologyDocument31 paginiHPEX 358-002 - Basics of EpidemiologyMichelle ValenzuelaÎncă nu există evaluări
- Hema2 Finalssssss PDFDocument8 paginiHema2 Finalssssss PDFMarcelino CalataÎncă nu există evaluări
- TN MRB Auxiliary Nurse Midwife Exam SyllabusDocument4 paginiTN MRB Auxiliary Nurse Midwife Exam SyllabusmathanbhuÎncă nu există evaluări
- Kertas Kerja Program Sayangkan KitaDocument5 paginiKertas Kerja Program Sayangkan Kitaaknb2702Încă nu există evaluări
- Headache: Differential Diagnosis of HeadacheDocument139 paginiHeadache: Differential Diagnosis of Headachemero1983Încă nu există evaluări
- Conjunctivitis A Systematic Review of Diagnosis and TreatmentDocument18 paginiConjunctivitis A Systematic Review of Diagnosis and TreatmentdasityarachmanÎncă nu există evaluări
- Care of Postpartum PatientsDocument35 paginiCare of Postpartum PatientsCHi NAi100% (1)
- List of Top Level Categories: CHAPTER 01 Certain Infectious or Parasitic DiseasesDocument148 paginiList of Top Level Categories: CHAPTER 01 Certain Infectious or Parasitic Diseasesျပည္ စိုးÎncă nu există evaluări
- Full List of Consortium Names and Affiliations Are Listed in The AppendixDocument60 paginiFull List of Consortium Names and Affiliations Are Listed in The AppendixJohnÎncă nu există evaluări
- COURSE OBJECTIVES or NursingDocument5 paginiCOURSE OBJECTIVES or NursingFil AquinoÎncă nu există evaluări
- M4 - Didactic - NCM 118Document4 paginiM4 - Didactic - NCM 118KARL FESARITÎncă nu există evaluări
- SEMINAR On New FilariaDocument50 paginiSEMINAR On New FilariaArun JvÎncă nu există evaluări
- Chapter 12 - Hypertension - Lost Shaker of Salt Level IIDocument6 paginiChapter 12 - Hypertension - Lost Shaker of Salt Level IIaleksme880% (1)
- Hemorrhage PathophysiologyDocument3 paginiHemorrhage PathophysiologyJubelle Sipalay0% (1)
- Heparin - ClinicalKeyDocument85 paginiHeparin - ClinicalKeydayannaÎncă nu există evaluări
- LET Contacts 10-14Document4 paginiLET Contacts 10-14Wayne MaughanÎncă nu există evaluări
- Methylene Blue For Refractory Shock in Pediatric PatientsDocument16 paginiMethylene Blue For Refractory Shock in Pediatric Patientsandi rahmatÎncă nu există evaluări
- Research Project ProposalDocument8 paginiResearch Project ProposalAthena Irish LastimosaÎncă nu există evaluări
- Gastro Review QuestionsDocument9 paginiGastro Review QuestionsPortia Dulce Patatag ToqueroÎncă nu există evaluări
- Goiter: What Is The Thyroid Gland?Document2 paginiGoiter: What Is The Thyroid Gland?Julio LeviÎncă nu există evaluări
- TFCBT Training GuidelinesDocument3 paginiTFCBT Training GuidelinespolÎncă nu există evaluări
- Reckettsia and ChlamediaDocument37 paginiReckettsia and ChlamediaMuqtadir “The Ruler” KuchikiÎncă nu există evaluări
- Sedatives, Hypnotics & Anxiolytics (Antianxiety Drugs) Ms. S.R.DhandeDocument347 paginiSedatives, Hypnotics & Anxiolytics (Antianxiety Drugs) Ms. S.R.DhandeEsha pantÎncă nu există evaluări