S-ar putea să vă placă și
- Pharmacology of Diuretics: DR - Datten Bangun MSC, SPFKDocument46 paginiPharmacology of Diuretics: DR - Datten Bangun MSC, SPFKRizky Pramata Simamora 19000029Încă nu există evaluări
- CVS - DiureticsDocument8 paginiCVS - Diureticshlouis8Încă nu există evaluări
- Chapter 3 CVS & RenalDocument116 paginiChapter 3 CVS & RenalKIDUS YAREDÎncă nu există evaluări
- Diuretics 1Document34 paginiDiuretics 1ياسمين مجديÎncă nu există evaluări
- DR - Datten Bangun MSC, SPFK: Dept - Farmakologi & Therapeutik Fak - Kedokteran UhnDocument39 paginiDR - Datten Bangun MSC, SPFK: Dept - Farmakologi & Therapeutik Fak - Kedokteran UhnTeus FatamorganaÎncă nu există evaluări
- Chapter 18 DIURETICSDocument14 paginiChapter 18 DIURETICSAlexandra AlexaÎncă nu există evaluări
- DiureticsDocument12 paginiDiureticslandita683Încă nu există evaluări
- Diuretics: Haitham Mahmood AlwaliDocument32 paginiDiuretics: Haitham Mahmood Alwaligaurav adhikariÎncă nu există evaluări
- Dr. Prajogo - PharmacologyDocument144 paginiDr. Prajogo - Pharmacologydelia rahmaÎncă nu există evaluări
- Diuretics: Pranjal Wagh Master of Pharmacy (2021-2023) Poona College of PharmacyDocument39 paginiDiuretics: Pranjal Wagh Master of Pharmacy (2021-2023) Poona College of PharmacyPranjalÎncă nu există evaluări
- Diuretic Drugs Dr. DarmawanDocument54 paginiDiuretic Drugs Dr. DarmawanEdi KurniadiÎncă nu există evaluări
- DiureticsDocument29 paginiDiureticsdeepak askarÎncă nu există evaluări
- Diuretics: Professor C. B. Choudhary Department of Pharmacology NMCTH, BiratnagarDocument52 paginiDiuretics: Professor C. B. Choudhary Department of Pharmacology NMCTH, BiratnagarKulgaurav RegmiÎncă nu există evaluări
- c15 Diuretic AgentsDocument13 paginic15 Diuretic AgentsmohammadÎncă nu există evaluări
- Ph'cology of Diuretics (RZH)Document48 paginiPh'cology of Diuretics (RZH)beby febyola siagianÎncă nu există evaluări
- UntitledDocument59 paginiUntitledSafayet HossainÎncă nu există evaluări
- Classification of DiureticsDocument23 paginiClassification of DiureticsBeryl MarshallÎncă nu există evaluări
- Pharmacology I, Diuretics NK-modified 2Document32 paginiPharmacology I, Diuretics NK-modified 289c8g7bvvvÎncă nu există evaluări
- Diuretics: Diuretics Are Drugs That Increase The Volume of Urine FlowDocument35 paginiDiuretics: Diuretics Are Drugs That Increase The Volume of Urine FlowAmanuel Maru100% (1)
- Genitourinary PharmacologyDocument11 paginiGenitourinary PharmacologySadia YousafÎncă nu există evaluări
- Beige Brown Vintage Group Project Presentation - 20230922 - 184226 - 0000Document25 paginiBeige Brown Vintage Group Project Presentation - 20230922 - 184226 - 0000Mercurio AysonÎncă nu există evaluări
- 25.9 Regulation of Fluid Volume and Composition - Anatomy and Physiology 2e - OpenStaxDocument4 pagini25.9 Regulation of Fluid Volume and Composition - Anatomy and Physiology 2e - OpenStaxMarlene AngwaforÎncă nu există evaluări
- Diuretics TableDocument5 paginiDiuretics TableLaylee ClareÎncă nu există evaluări
- DiureticsDocument10 paginiDiureticsSantosh RoyÎncă nu există evaluări
- 6-Drugs Acting On The Renal System - 2Document65 pagini6-Drugs Acting On The Renal System - 2Hamid Hussain HamidÎncă nu există evaluări
- Diuretics For CardiacDocument6 paginiDiuretics For CardiacBetsy Brown ByersmithÎncă nu există evaluări
- Rational Use of Diuretics and Pathophysiology of Edema: OP Kalra, Amitesh AggarwalDocument10 paginiRational Use of Diuretics and Pathophysiology of Edema: OP Kalra, Amitesh AggarwalVina AnasthasiaÎncă nu există evaluări
- Diuretics and Dialysis: DR Arpana HazarikaDocument104 paginiDiuretics and Dialysis: DR Arpana HazarikaArpana HazarikaÎncă nu există evaluări
- Lecture 6-1Document50 paginiLecture 6-1Vijita PriyaÎncă nu există evaluări
- Diuretics: BY-DR. Saurabh Kansal Dept. of Pharmacology Msy Medical College MeerutDocument33 paginiDiuretics: BY-DR. Saurabh Kansal Dept. of Pharmacology Msy Medical College MeerutPrakhar GoelÎncă nu există evaluări
- Renal Drugs Diuretics Agents: by Desalegn Chilo (B.Pharm, MSC)Document54 paginiRenal Drugs Diuretics Agents: by Desalegn Chilo (B.Pharm, MSC)Remedan TahaÎncă nu există evaluări
- Diuretics: By: Prof. A. AlhaiderDocument33 paginiDiuretics: By: Prof. A. AlhaiderNina KerafÎncă nu există evaluări
- #DiureticsDocument48 pagini#DiureticsRuturaj DesaiÎncă nu există evaluări
- General Principles of Tubular ReabsorptionDocument54 paginiGeneral Principles of Tubular ReabsorptionRalph JacintoÎncă nu există evaluări
- Diuretics and Anti Diuretics: Year Iii Pharm.D Dr. V. ChitraDocument49 paginiDiuretics and Anti Diuretics: Year Iii Pharm.D Dr. V. ChitranikithaÎncă nu există evaluări
- NA 01 - Renal PathophysiologyDocument8 paginiNA 01 - Renal PathophysiologyMaggie CacieÎncă nu există evaluări
- Obat Pada Ginjal: Prof M.A.Widodo PHDDocument53 paginiObat Pada Ginjal: Prof M.A.Widodo PHDPriiya Ashiwini100% (1)
- Renal Note On DiureticsDocument12 paginiRenal Note On DiureticsLilian EdeniÎncă nu există evaluări
- Diuretic DrugsDocument2 paginiDiuretic DrugsEngku ElisaÎncă nu există evaluări
- Cardiovascular For PharmacologDocument134 paginiCardiovascular For Pharmacologephremtigabie7Încă nu există evaluări
- Part 1 - US-Grade 4-BiochemistryDocument34 paginiPart 1 - US-Grade 4-BiochemistryFarah Bashar Al-RawachyÎncă nu există evaluări
- Diuretics MergedDocument727 paginiDiuretics MergedRinkiÎncă nu există evaluări
- Filtration at Rest: Retention of WaterDocument19 paginiFiltration at Rest: Retention of WaterkoushiksarkerÎncă nu există evaluări
- Lecture+24 +25+diureticsDocument69 paginiLecture+24 +25+diureticsGhina RizwanÎncă nu există evaluări
- Diuretics: Gilbert S 2014Document34 paginiDiuretics: Gilbert S 2014Josephine SÎncă nu există evaluări
- Drugs Affecting Renal SystemDocument58 paginiDrugs Affecting Renal SystemDaniel OkakaÎncă nu există evaluări
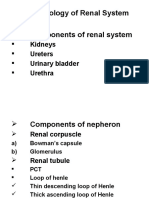
- Pharmacology of Renal System Components of Renal System: Kidneys Ureters Urinary Bladder UrethraDocument30 paginiPharmacology of Renal System Components of Renal System: Kidneys Ureters Urinary Bladder UrethraMirza HassanÎncă nu există evaluări
- ThiazideDocument4 paginiThiazideEkarthi KeyanÎncă nu există evaluări
- "Natriuresis": Prepared by Dr. Hala Zaqout 1Document89 pagini"Natriuresis": Prepared by Dr. Hala Zaqout 1Ahmed FouadÎncă nu există evaluări
- DiureticsDocument58 paginiDiureticsabenezergebrekirstosÎncă nu există evaluări
- Pathogenesis, Diagnosis and Management of Hyperkalemia PDFDocument9 paginiPathogenesis, Diagnosis and Management of Hyperkalemia PDFJbarrianÎncă nu există evaluări
- Diuretics and Renal HormonesDocument3 paginiDiuretics and Renal Hormoneswahyu PurÎncă nu există evaluări
- Diuretics: Chris Hague, PHDDocument29 paginiDiuretics: Chris Hague, PHDranachamanÎncă nu există evaluări
- Diuretic DrugsDocument62 paginiDiuretic DrugsAbdul WahabÎncă nu există evaluări
- Renal UWDocument7 paginiRenal UWridin007Încă nu există evaluări
- Diuretics: DR Sindwa KanyimbaDocument43 paginiDiuretics: DR Sindwa Kanyimbaedward kaumbaÎncă nu există evaluări
- ReferatDocument53 paginiReferatHendri SaputraÎncă nu există evaluări
- Dangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiaDocument7 paginiDangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiagorodoeÎncă nu există evaluări
- Urinary Stones: Medical and Surgical ManagementDe la EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoÎncă nu există evaluări
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansDe la EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpÎncă nu există evaluări
- Acute Promyelocytic LeukemiaDocument16 paginiAcute Promyelocytic LeukemiaMoataz TrabehÎncă nu există evaluări
- Ghicavîi Victor: - Name: Creliciuc Maria - Age: 64ani (15/04/1949) - Location: KishinauDocument30 paginiGhicavîi Victor: - Name: Creliciuc Maria - Age: 64ani (15/04/1949) - Location: KishinauMoataz TrabehÎncă nu există evaluări
- 5 Reticuolocyte CountDocument11 pagini5 Reticuolocyte CountMoataz TrabehÎncă nu există evaluări
- RE-DUAL PCI: Dual Antithrombotic Therapy With Dabigatran After Percutaneous Coronary Intervention in Patients With Atrial FibrillationDocument20 paginiRE-DUAL PCI: Dual Antithrombotic Therapy With Dabigatran After Percutaneous Coronary Intervention in Patients With Atrial FibrillationMoataz TrabehÎncă nu există evaluări
- Corticosteroids For Treatment of Sore Throat: Systematic Review and Meta-Analysis of Randomised Trials BMJ 2017Document13 paginiCorticosteroids For Treatment of Sore Throat: Systematic Review and Meta-Analysis of Randomised Trials BMJ 2017Moataz TrabehÎncă nu există evaluări
- English Tests For Infectious DiseasesDocument82 paginiEnglish Tests For Infectious DiseasesMoataz TrabehÎncă nu există evaluări
- TTTTDocument26 paginiTTTTMoataz TrabehÎncă nu există evaluări
- 8 - Anti Allergic DrugsDocument8 pagini8 - Anti Allergic DrugsMoataz TrabehÎncă nu există evaluări
- B-Selective: I Group: Nonsteroidal Anti-Inflammatory Drugs (Nonsteroidal Ntiinflammatory)Document6 paginiB-Selective: I Group: Nonsteroidal Anti-Inflammatory Drugs (Nonsteroidal Ntiinflammatory)Moataz TrabehÎncă nu există evaluări
- 13 - Antibiotic III Nalidixic AcidDocument7 pagini13 - Antibiotic III Nalidixic AcidMoataz TrabehÎncă nu există evaluări
- PediatricsDocument84 paginiPediatricsMoataz TrabehÎncă nu există evaluări
- 5 Digestive IDocument11 pagini5 Digestive IMoataz TrabehÎncă nu există evaluări
- 05.psychiatry Fixed by E.G E.KDocument54 pagini05.psychiatry Fixed by E.G E.KMoataz Trabeh100% (1)
- Imle A 03 03 2015Document82 paginiImle A 03 03 2015Moataz TrabehÎncă nu există evaluări
- Blueprints QA Pediatrics For Step 3 1Document59 paginiBlueprints QA Pediatrics For Step 3 1Moataz Trabeh100% (1)
- AnatomDocument11 paginiAnatomDragan DragovicÎncă nu există evaluări
- Essentials 4eDocument874 paginiEssentials 4eJehada AbdukadilÎncă nu există evaluări
- Fluids and Electrolytes A Fast and Easy Way To Understand Acid-Base Balance Without MemorizationDocument195 paginiFluids and Electrolytes A Fast and Easy Way To Understand Acid-Base Balance Without MemorizationNayely MoralesÎncă nu există evaluări
- AUBFDocument32 paginiAUBFAndrei Tumarong AngoluanÎncă nu există evaluări
- Urogenital Guide Notes PDFDocument26 paginiUrogenital Guide Notes PDFJoryn LimÎncă nu există evaluări
- Human and Social Biology 5096 GCE O Level For Examination in 2008Document26 paginiHuman and Social Biology 5096 GCE O Level For Examination in 2008mstudy123456Încă nu există evaluări
- Anatomy MCQsDocument22 paginiAnatomy MCQsRashid Hussain89% (9)
- Internal Medicine - CardiologyDocument122 paginiInternal Medicine - CardiologySoleil Daddou100% (2)
- The Urinary System Overview of Kidney FunctionsDocument9 paginiThe Urinary System Overview of Kidney FunctionsLALRINTLUANGI CHHAKCHHUAKÎncă nu există evaluări
- Biopharmaceutics and PharmacokineticsDocument76 paginiBiopharmaceutics and PharmacokineticsEswar Gupta Maddi100% (4)
- Renal Function TestsDocument10 paginiRenal Function TestsVirendraÎncă nu există evaluări
- Renal MCQs (2017), Dr. Ahmad AlarabiDocument24 paginiRenal MCQs (2017), Dr. Ahmad AlarabiAziz50% (2)
- Guyton & Hall Physio: Chapter 26 Urine Formation by The KidneysDocument66 paginiGuyton & Hall Physio: Chapter 26 Urine Formation by The KidneysMedSchoolStuff90% (21)
- Fluid and Electrolyte TherapyDocument23 paginiFluid and Electrolyte TherapyJamal ArizonaÎncă nu există evaluări
- Renal Function Tests 1 PDFDocument56 paginiRenal Function Tests 1 PDFCharles Bryahn OkoboiÎncă nu există evaluări
- How Urine Is Formed?Document6 paginiHow Urine Is Formed?DARRYL JOY ALCALAÎncă nu există evaluări
- Urinary System TermDocument30 paginiUrinary System TermRhahima SyafrilÎncă nu există evaluări
- Renal Physiology: Structure & Function of Kidneys and Urinary System, Renal Processes and MicturitionDocument21 paginiRenal Physiology: Structure & Function of Kidneys and Urinary System, Renal Processes and MicturitionSufyan MirzaÎncă nu există evaluări
- Renal Quiz (12.8.2017)Document3 paginiRenal Quiz (12.8.2017)HardiTariqHammaÎncă nu există evaluări
- For Website All Questions PDFDocument26 paginiFor Website All Questions PDFAyyaz HussainÎncă nu există evaluări
- Counter Current MechanismDocument39 paginiCounter Current MechanismRAGHUNANDAN R100% (2)
- Excretory Products and Their Elimination: SolutionsDocument10 paginiExcretory Products and Their Elimination: SolutionsEkta ManglaniÎncă nu există evaluări
- Anatomy and PhysiologyDocument37 paginiAnatomy and PhysiologyJamesMarcoMÎncă nu există evaluări
- Renal MCQ 2Document6 paginiRenal MCQ 2AzizÎncă nu există evaluări
- Pharmacokinetic and Pharmacodynamic Principles For ToxicologyDocument12 paginiPharmacokinetic and Pharmacodynamic Principles For ToxicologyMARIA TELLEZÎncă nu există evaluări
- Ureter AnatomyDocument8 paginiUreter AnatomyGhaly AmirÎncă nu există evaluări
- Life Processes 2Document30 paginiLife Processes 2Generic nameÎncă nu există evaluări
- Chapter 41 - Osmotic Regulation and ExcretionDocument18 paginiChapter 41 - Osmotic Regulation and ExcretioniavahhoÎncă nu există evaluări
- Drug Use in Special Conditions - CLD and CKDDocument93 paginiDrug Use in Special Conditions - CLD and CKDadamu mohammadÎncă nu există evaluări
- Drug MetabolismDocument52 paginiDrug MetabolismUsman AkhtarÎncă nu există evaluări