S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- 20121605171139Document3.240 pagini20121605171139Ainun Marfu' LailyÎncă nu există evaluări
- Imesa Brochure Dryer Es34Document3 paginiImesa Brochure Dryer Es34Rakhmad SucahyoÎncă nu există evaluări
- Analisis Tingkat Kepuasan Pelanggan Dengan Menggunakan Metode Customer Satisfaction Index Dan ImportanceDocument9 paginiAnalisis Tingkat Kepuasan Pelanggan Dengan Menggunakan Metode Customer Satisfaction Index Dan ImportanceRakhmad SucahyoÎncă nu există evaluări
- RCA CompleteDocument68 paginiRCA CompleteRakhmad Sucahyo100% (1)
- Guidance For Performing Failure Mode and Effects Analysis With Performance Improvement ProjectsDocument14 paginiGuidance For Performing Failure Mode and Effects Analysis With Performance Improvement ProjectsRakhmad SucahyoÎncă nu există evaluări
- Perhitungan Net Present Value: Cash FlowDocument1 paginăPerhitungan Net Present Value: Cash FlowRakhmad SucahyoÎncă nu există evaluări
- Middle East Respiratory Syndrome - Corona Virus: Pedoman Umum Kesiapsiagaan MenghadapiDocument1 paginăMiddle East Respiratory Syndrome - Corona Virus: Pedoman Umum Kesiapsiagaan MenghadapiRakhmad SucahyoÎncă nu există evaluări
- Priority Scoring Tool July 2010Document1 paginăPriority Scoring Tool July 2010Rakhmad SucahyoÎncă nu există evaluări
- Perhitungan Net Present Value: Cash Flow With The Old X-Ray MachineDocument2 paginiPerhitungan Net Present Value: Cash Flow With The Old X-Ray MachineRakhmad SucahyoÎncă nu există evaluări
- InfectionDocument16 paginiInfectionRakhmad SucahyoÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- US Hex Bolt SizesDocument2 paginiUS Hex Bolt SizesYana Jarang OlÎncă nu există evaluări
- Wood Magazine Issue #189Document96 paginiWood Magazine Issue #189bangbang63100% (1)
- 545 ELP-ES-2011 - Catálogo de DisipadoresDocument24 pagini545 ELP-ES-2011 - Catálogo de DisipadoresrichkidÎncă nu există evaluări
- VocationalDocument2 paginiVocationalMegha RoyÎncă nu există evaluări
- C32 Electronic Unit Injector - Adjust PDFDocument4 paginiC32 Electronic Unit Injector - Adjust PDFmanu luvunga100% (2)
- Catalogo Bulldog Jgo Empacaduras Maquinas+Motores Todo en UnoDocument78 paginiCatalogo Bulldog Jgo Empacaduras Maquinas+Motores Todo en UnoAlexis SanchezÎncă nu există evaluări
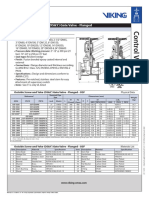
- Outside Screw and Yoke (OS&Y) Gate Valve - Flanged: Technical FeaturesDocument2 paginiOutside Screw and Yoke (OS&Y) Gate Valve - Flanged: Technical FeaturesMark Louie GuintoÎncă nu există evaluări
- GeomediaDocument37 paginiGeomediaEdilson MahumaneÎncă nu există evaluări
- 2015 VGP Checklist - Rev0Document9 pagini2015 VGP Checklist - Rev0Takis RappasÎncă nu există evaluări
- Hot Water Recirculation PumpsDocument22 paginiHot Water Recirculation Pumpsniaz kilamÎncă nu există evaluări
- Development of Rotary Weeder Blades by Finite Element MethodDocument5 paginiDevelopment of Rotary Weeder Blades by Finite Element MethodijsretÎncă nu există evaluări
- 101.S-4501 Steamer Cyclone Cleaning ProcedureDocument6 pagini101.S-4501 Steamer Cyclone Cleaning ProcedureTRONGKIMÎncă nu există evaluări
- Polymers For Transdermal Drug Delivery SystemsDocument9 paginiPolymers For Transdermal Drug Delivery SystemsAmjadRazaÎncă nu există evaluări
- How To Fix - External Disk Drive Suddenly Became RAWDocument96 paginiHow To Fix - External Disk Drive Suddenly Became RAWAntonio Marcano0% (1)
- Use of Multimeter TextDocument76 paginiUse of Multimeter Textprueba1100% (2)
- PPAPDocument2 paginiPPAPVlad NitaÎncă nu există evaluări
- Trouble Codes C32Document10 paginiTrouble Codes C32AliHabes100% (2)
- Pile Cap Design 4pilesDocument6 paginiPile Cap Design 4pilesabshawÎncă nu există evaluări
- Thermofisher U01316-R2-Gp-Precision-Baths PDFDocument73 paginiThermofisher U01316-R2-Gp-Precision-Baths PDFelduÎncă nu există evaluări
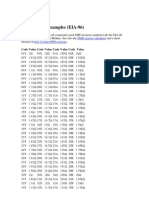
- SMD Resistor ExamplesDocument5 paginiSMD Resistor Examplesmarcbuss100% (1)
- ManualDocument9 paginiManualRonit DattaÎncă nu există evaluări
- Flight DynamicsDocument57 paginiFlight DynamicsDexto100% (2)
- Software Hardware ListDocument2 paginiSoftware Hardware ListjackÎncă nu există evaluări
- Procurement Guideline For ATL SchoolsDocument4 paginiProcurement Guideline For ATL SchoolsManKapÎncă nu există evaluări
- Caustic CrackingDocument17 paginiCaustic CrackingDurga PrasadÎncă nu există evaluări
- Advanced Techniques in Power System Protective Relaying PDFDocument332 paginiAdvanced Techniques in Power System Protective Relaying PDFshashikant yadavÎncă nu există evaluări
- Hela Bojuna - Comparative StatementDocument27 paginiHela Bojuna - Comparative StatementNadeeshani MunasingheÎncă nu există evaluări
- Manual Kls MartinDocument27 paginiManual Kls MartinChris AliÎncă nu există evaluări
- CFD Analysis of First Stage Nozzle Cooling Optimization in Gas TurbinesDocument7 paginiCFD Analysis of First Stage Nozzle Cooling Optimization in Gas TurbinesMahmood ElnagarÎncă nu există evaluări
- Sensores AvDocument12 paginiSensores Avhb CorpÎncă nu există evaluări